Yonsei Med J.
2009 Apr;50(2):195-199.
An Evaluation of Glucose Tolerance in Essential Hypertension
- Affiliations
-
- 1Endocrinology Section, Department of Internal Medicine, Trakya University Medical Faculty, Edirne, Turkey. aatugrul@yahoo.co.uk
Abstract
- PURPOSE
This study aimed to determine the impaired glucose tolerance and diabetes prevalence in patients with essential hypertension (HT) and to compare the developed microvascular complications of these groups. MATERIALS AND METHODS: An oral glucose tolerance test (OGTT) was performed on 338 essential hypertensive cases and glucose tolerances were classified according to ADA-2002 criteria. RESULTS: Of the 338 cases, 32 people had diabetes (DM, 9.46%), 78 people had glucose intolerance (IGT, 23.1%), and 228 people had only hypertension but not IGT and DM (67.4%). Both the mean ages of the DM group (56.9 +/- 6.7 years, p = 0.002) and IGT group (56.3 +/- 8.4 years, p = 0.003) were older than the mean age of the control group (51.1 +/- 6.4 years). The risk of IGT development was found to be four times greater in male cases than female cases when compared to the control group (p = 0.004, add ratio = 4.194). There were no significant differences in the body mass indexes (BMI's), hypertension durations, and microvascular complications between the groups. CONCLUSION: In conclusion, the risk of IGT and DM development in hypertensive cases increases with aging and longer hypertension duration. The risk of IGT development in hypertensive cases is four times more in males.
MeSH Terms
Figure
-
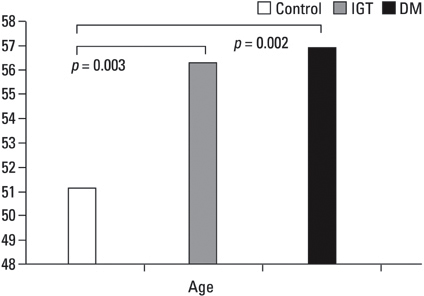
Fig. 1 Mean ages of three groups. IGT, impaired glucose tolerance; DM, diabetes mellitus.
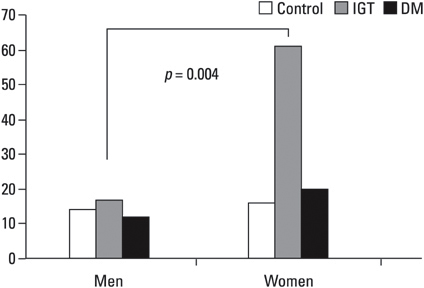
Fig. 2 Number of male and female subjects in three groups. IGT, impaired glucose tolerance; DM, diabetes mellitus.
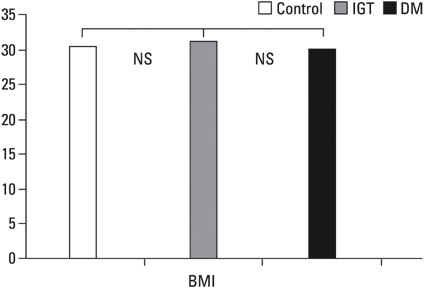
Fig. 3 Means of BMI of three groups. IGT, impaired glucose tolerance; DM, diabetes mellitus; BMI, body mass index; NS, statistically non-significant.

Fig. 4 Duration of hypertension in three groups. IGT, impaired glucose tolerance; DM, diabetes mellitus; NS, statistically non-significant.
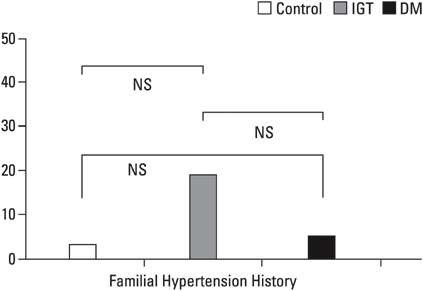
Fig. 5 Number of patients having a familial hypertension history in three groups. IGT, impaired glucose tolerance; DM, diabetes mellitus; NS, statistically non-significant.
Reference
-
1. Pereira MA, Jacobs DR Jr, Van Horn L, Slattery ML, Kartashov AI, Ludwig DS. Dairy comsumption, obesity, and the insulin resistance syndrome in young adults: the CARDIA Study. JAMA. 2002. 287:2081–2089.
Article2. Natalucci S, Boemi M, Fumelli P, Testa I, Fumelli D, Burattini R. One- and two- compartment minimal models detect similar alterations of glucose metabolism indexes in hypertension. Metabolism. 2000. 49:1529–1536.3. Gouveia LM, Paccola GM, Torquato MT, Menezes FO, Piccinato CE, Foss MC. Peripheral glucose metabolism in patients with essential hypertension. Horm Metab Res. 2000. 32:35–39.
Article4. American Diabetes Association. Screening for type 2 diabetes. Diabetes Care. 2002. 25:Suppl 1. S21–S24.5. von Eckardstein A, Schulte H, Assmann G. Risk for diabetes mellitus in middle-aged Caucasian male participants of the PROCAM study: implications for the definition of impaired fasting glucose by the American Diabetes Association. Prospective cardiovascular Münster. J Clin Endocrinol Metab. 2000. 85:3101–3108.
Article6. Dunstan DW, Zimmet PZ, Welborn TA, De Courten MP, Cameron AJ, Sicree RA, et al. The rising prevalence of diabetes and impaired glucose tolerance: the Australian Diabetes, Obesity and Lifestyle Study. Diabetes Care. 2002. 25:829–834.7. Knowler WC, Barrett-Connor E, Fowler SE, Hamman RF, Lachin JM, Walker EA, et al. Reduction in the incidence of type 2 diabetes with lifestyle intervention or metformin. N Engl J Med. 2002. 346:393–403.
Article8. Tuomilehto J, Lindström J, Eriksson JG, Valle TT, Hämäläinen H, Ilanne-Parikka P, et al. Prevention of type 2 diabetes mellitus by changes in lifestyle among subjects with impaired glucose tolerance. N Engl J Med. 2001. 344:1343–1350.
Article9. Barzilay JI, Spiekerman CF, Kuller LH, Burke GL, Bittner V, Gottdiener JS, et al. Prevalence of clinical and isolated subclinical cardiovascular disease in older adults with glucose disorders: the Cardiovascular Health Study. Diabetes Care. 2001. 24:1233–1239.
Article10. Rodriguez BL, Abbott RD, Fujimoto W, Waitzfelder B, Chen R, Masaki K, et al. The American Diabetes Association and World Health Organization classifications for diabetes: their impact on diabetes prevalence and total and cardiovascular disease mortality in elderly Japanese-American men. Diabetes Care. 2002. 25:951–955.
Article11. Lim SC, Tai ES, Tan BY, Chew SK, Tan CE. Cardiovascular risk profile in individuals with borderline glycemia: the effect of the 1997 American Diabetes Association diagnostic criteria and the 1998 World Health Organization Provisional Report. Diabetes Care. 2000. 23:278–282.
Article12. Shaw JE, Zimmet PZ, Hodge AM, de Courten M, Dowse GK, Chitson P, et al. Impaired fasting glucose: how low should it go? Diabetes Care. 2000. 23:34–39.
Article13. Borde-Perry WC, Campbell KL, Murtaugh KH, Gidding S, Falkner B. The association between hypertension and other cardiovascular risk factors in young adult African Americans. J Clin Hypertens (Greenwich). 2002. 4:17–22.
Article14. Simon NR, Frishman WH. Diabetes mellitus in the aging: epidemiologic and therapeutic considerations. Am J Geriatr Cardiol. 1992. 1:22–36.15. King H, Djumaeva S, Abdullaev B, Gacic Dobo M. Epidemiology of glucose intolerance and associated factors in Uzbekistan: a survey in Sirdaria province. Diabetes Res Clin Pract. 2002. 55:19–27.
Article16. Lam TH, Liu LJ, Janus ED, Lam KS, Hedley AJ. Hong Kong Cardiovascular Risk Factor Prevalence Study Steering Committee. Fibrinogen, other cardiovascular risk factors and diabetes mellitus in Hong Kong: a community with high prevalence of type 2 diabetes mellitus and impaired glucose tolerance. Diabet Med. 2000. 17:798–806.
Article17. Hanefeld M, Koehler C, Henkel E, Fuecker K, Schaper F, Temelkova-Kurktschiev T. Post-challenge hyperglycaemia relates more strongly than fasting hyperglycaemia with carotid intima-media thickness: the RIAD Study. Risk Factors in Impaired Glucose Tolerance for Atherosclerosis and Diabetes. Diabet Med. 2000. 17:835–840.
Article18. Ribstein J, Du Cailar G, Mimran A. Glucose tolerance and age-associated dacline in renal function of hypertensive patients. J Hypertens. 2001. 19:2257–2264.
Article19. Satman I, Yilmaz T, Sengül A, Salman S, Salman F, Uygur S, et al. Population-based study of diabetes and risk characteristics in Turkey: results of the turkish diabetes epidemiology study (TURDEP). Diabetes Care. 2002. 25:1551–1556.20. Ozkan Y, Donder E, Dogan H, Demir A, YalnIz M, Sokmen S. Hipertansif hastalarda tip 2 diabetes mellitus ve bozulmus glukoz tolerans sIklIgI. Turkish Journal of Endocrinology and Metabolism. 1999. 3(2):Suppl 1. 129.21. Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the Expert Committee on the diagnosis and classification of diabetes mellitus. Diabetes Care. 2002. 25:Suppl 1. S5–S20.22. Ribstein J, Du Cailar G, Mimran A. Glucose tolerance and age-associated decline in renal function of hypertensive patients. J Hypertens. 2001. 19:2257–2264.
Article23. Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B, Allen K, et al. Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. N Engl J Med. 2002. 346:802–810.
Article24. Tomiyama H, Kimura Y, Okazaki R, Kushiro T, Abe M, Kuwabara Y, et al. Close relationship of abnormal glucose tolerance with endotheliel dysfunction in hypertension. Hypertension. 2000. 36:245–249.
Article25. Gabir MM, Hanson RL, Dabelea D, Imperatore G, Roumain J, Bennett PH, et al. Plasma glucose and prediction of microvascular disease and mortality: evaluation of 1997 American Diabetes Association and 1999 World Health Organization criteria for diagnosis of diabetes. Diabetes Care. 2000. 23:1113–1118.
Article26. Meigs JB, D'Agostinsr RB, Nathan DM, Rifai N, Wilson PW. Framingham Offspring Study. Longitudinal association of glycemia and microalbuminuria; the Framingham Offspring Study. Diabetes Care. 2002. 25:977–983.27. Sosenko JM, Hu D, Welty T, Howard BV, Lee E, Robbins DC. Albuminuria in recent-onset type 2 diabetes. Diabetes Care. 2002. 25:1078–1084.
Article28. Isomaa B, Almgren P, Tuomi T, Forsén B, Lahti K, Nissén M, et al. Cardiovascular morbidity and mortality associated with the metabolic syndrome. Diabetes Care. 2001. 24:683–689.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evaluation of Glucone Tolerance and Insulin Secretion in Two Patients with Primary Hyperparathyroidism Before and After Surgery
- Letter: Normal Glucose Tolerance with a High 1-Hour Postload Plasma Glucose Level Exhibits Decreased beta-Cell Function Similar to Impaired Glucose Tolerance (Diabetes Metab J 2015;39:147-53)
- Prevalence of Diabetes Mellitus and Associated Diseases in Yeungnam Province Area
- Predictive capability of fasting-state glucose and insulin measurements for abnormal glucose tolerance in women with polycystic ovary syndrome
- Insulin Resistance in Middle Aged Normotensive Offspring of the Hypertensive Parents in Korea
