Management of Melorheostosis
- Affiliations
-
- 1Department of Orthopedic Surgery, Chonnam National University Medical School, Gwangju, Korea. stjung@chonnam.ac.kr
- KMID: 2393519
- DOI: http://doi.org/10.4055/jkoa.2017.52.5.453
Abstract
- Melorheostosis is a very rare sclerosing bone disease with pain, joint stiffness, and limitation of motion. Its characteristic on radiography is a dense bone formation along the side of the bone, resembling the flow of candle grease. Various conservative or surgical methods have been practiced in treating pain and deformities. This is a report on the successful treatment result of six cases of melotheostosis, involving the metatarsal, metacarpal, clavicle, and tibia, which weretreated by conservative and operative treatment methods.
Keyword
MeSH Terms
Figure
-
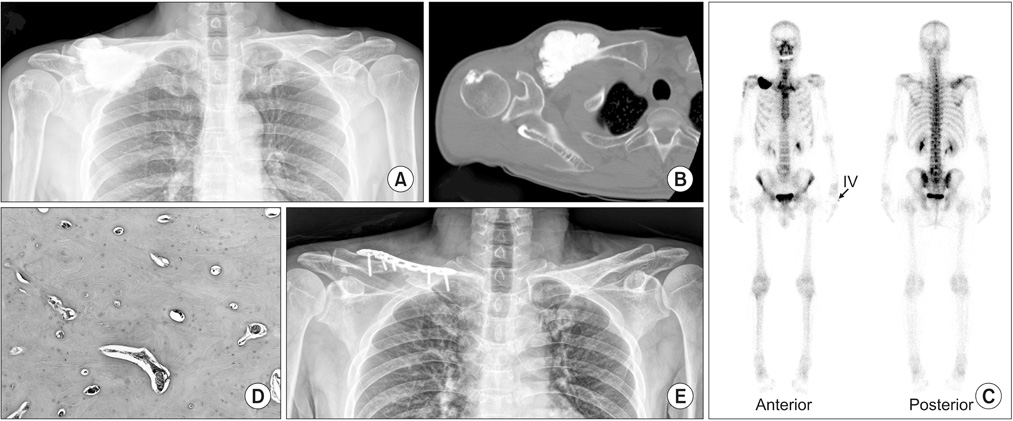
Figure 1 A 55-year-old male visited a hospital with palpable mass and pain on the right clavicular area. (A) Plain radiographs shows irregular cortical hyperostosis and intracortical lesions involving the right distal clavicle and lateral cortex of proximal humerus. (B) Computed tomography shows a dense sclerotic change in the right distal clavicle and lateral cortex of proximal humerus. Moreover, a lobulated dense ossified mass was projected to an anteroinferior aspect of the right clavicle. (C) Whole body bone scan shows an increased activity corresponding to the sclerotic lesions site. (D) Histologic specimen disclosed bland immature bones with osteoblastic rimming, medullary fibrous tissue without inflammation, and fragmentated lamellar bones (H&E, ×200). (E) Postoperative radiographs show a complete removal of the lesion in right clavicle. IV, intravenous injection.

Figure 2 A 40-year-old male visited a hospital with palpable mass and pain on the right foot, near the 3rd and 4th metatarsal bone dorsal area. (A) Plain radiographs show irregular cortical hyperostosis and intracortical lesions involving the inferomedial calcaneus, inferior area of the cuboid and lateral cuneiform, on the 3rd and 4th metatarsal bases as well as the 3rd toe. (B) Whole body bone scan shows an increased activity corresponding to the sclerotic lesions site. (C) Histologic specimen revealing a markedly irregular bone with relatively little cellular activity. The marrow shows a mild fibrosis (H&E, ×200).

Figure 3 A 45-year-old male visited a hospital with palpable mass and intermittent pain on the right calf area. (A) Plain radiographs show an excessive osteosclerosis, involving the right tibia shaft, proximal tibia medial aspect, and distal femur medial aspect, especially dripping cangle wax appearance. (B) Magnetic resonance imaging shows a hypointensity signal on T1 and T2-weighted images. (C) Whole body bone scan shows an increased activity corresponding to the sclerotic lesions site. (D) Histologic specimen disclosed medullary fibrous tissue without inflammation, as well as thickened and sclerotic bony tracecula (H&E, ×40). (E) Postoperative radiographs shows partial excision of the lesion.

Figure 4 A 29-year-old male visited a hospital with palpable growing mass and pain on 4th finger of the left hand. (A, B) Plain radiographs and computed tomography shows osteosclerosis and hyperostosis involving the 4th finger, hamate, capitates, and the 3rd metatarsal bone. (C) Whole body bone scan shows an increased activity corresponding to the sclerotic lesions site. (D) Histologic specimen showed bland immature bones with osteoblastic rimming, medullary fibrous tissue without inflammation and fragmentated lamellar bones (H&E, ×100).
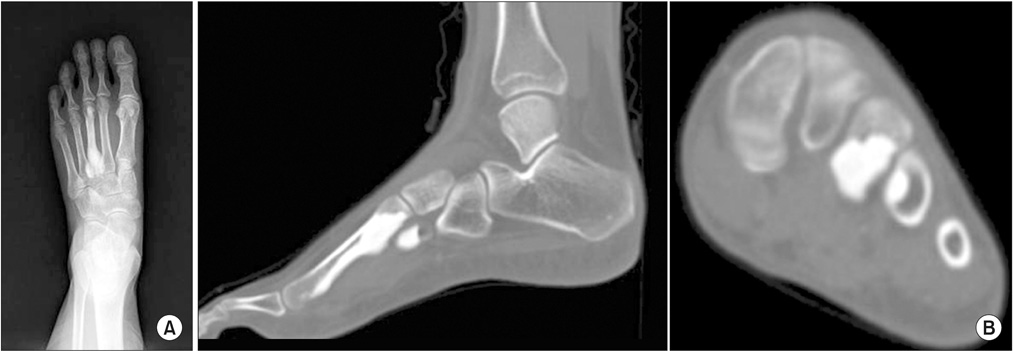
Figure 5 A 24-year-old female visited a hospital with incidentally detected sclerotic appearance on the left 3rd and 4th metatarsal bone. (A) Plain radiographs show a sclerotic change involving the 3rd metatarsal cortical bone and the 4th metatarsal bone basal area. (B) Computed tomography shows gross a sclerotic change and hypertrophy of cortical bone on the 3rd metatarsal bone as well as the regional sclerotic lesion on the 4th metatarsal bone base.

Figure 6 A 37-year-old female visited a hospital with palpable masses on the right calf proximal one third and distal one third area. (A) Plain radiographs show cortical hyperostosis and intracortical expansion, involving the right tibia anterior and medial aspects. (B) Computed tomography shows a sclerotic change in the right tibia anterior and medial aspects. (C) Whole body bone scan shows an increased activity corresponding to the sclerotic lesions site.
Reference
-
1. Gagliardi GG, Mahan KT. Melorheostosis: a literature review and case report with surgical considerations. J Foot Ankle Surg. 2010; 49:80–85.
Article2. Jain VK, Arya RK, Bharadwaj M, Kumar S. Melorheostosis: clinicopathological features, diagnosis, and management. Orthopedics. 2009; 32:512.
Article3. Leri A, Joanny J. Une affection non decrite des os: hyperostose ‘en coulee’ sur toute la longueur d' un membre ou ‘melorheostose’. Bull Mem Soc Med Hop Paris. 1922; 46:1141–1145.4. Campbell CJ, Papademetriou T, Bonfiglio M. Melorheostosis. A report of the clinical, roentgenographic, and pathological findings in fourteen cases. J Bone Joint Surg Am. 1968; 50:1281–1304.5. Freyschmidt J. Melorheostosis: a review of 23 cases. Eur Radiol. 2001; 11:474–479.
Article6. Younge D, Drummond D, Herring J, Cruess RL. Melorheostosis in children. Clinical features and natural history. J Bone Joint Surg Br. 1979; 61:415–418.
Article7. Jung ST, Jung SN, Lee KB. Melorheostosis of the foot. A case report. J Korean Orthop Assoc. 2000; 35:177–180.8. Greenspan A, Azouz EM. Bone dysplasia series. Melorheostosis: review and update. Can Assoc Radiol J. 1999; 50:324–330.9. Morris JM, Samilson RL, Corley CL. Melorheostosis. Review of the literature and report of an interesting case with a nineteen-year follow up. J Bone Joint Surg Am. 1963; 45:1191–1206.10. Slimani S, Nezzar A, Makhloufi H. Successful treatment of pain in melorheostosis with zoledronate, with improvement on bone scintigraphy. BMJ Case Rep. 2013; 2013. Published online June 21, 2013. DOI: 10.1136/bcr-2013-009820.
Article
