Korean J Obstet Gynecol.
2012 Oct;55(10):772-776.
A case of ovarian dysgerminoma with gonadal dysgenesis in 29-year-old woman with 46,XX karyotype
- Affiliations
-
- 1Department of Obstetrics and Gynecology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. soyeon.yoon@samsung.com
- 2Department of Pathology, Ilsin Christian Hospital, Busan, Korea.
- 3Department of Obstetrics and Gynecology, Ilsin Christian Hospital, Busan, Korea.
Abstract
- Gonadal dysgenesis occurs in rare case of ovarian tumor. Most tumors associated with gonadal dysgenesis were gonadoblastomas and dysgerminomas. In addition, premature ovarian insufficiency associated with these ovarian tumors in normal chromosomal type had not reported in many cases. A 29-year-old nulligravida woman who was concurrented with ovarian dysgerminoma and fibroma is presented. Measurements were made on serum lactate dehydrogenase, CA-125, CA 19-9 and pelvis ultrasonography and computed tomography. The clinical stage was IA and right salpingo-oophorectomy and wedge resection of the left ovary were done. On laboratory finding after operation on her serum follicular stimulating hormone was increased and E2 was decreased. The result of chromosomal analysis was 46,XX, normal. We represent here with brief review of literature one case of gonadal dysgenesis in nulligravida woman, associated with dysgerminoma, with normal karyotype.
Keyword
MeSH Terms
Figure
-
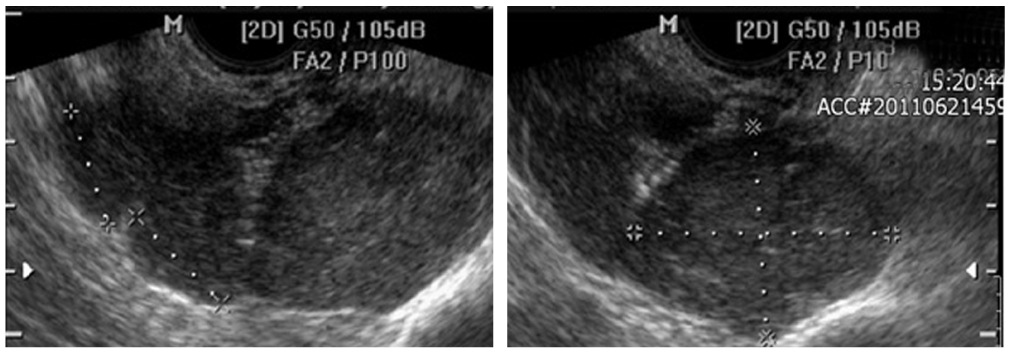
Fig. 1 Right ovarian tumor finding: transvaginal ultrasound.
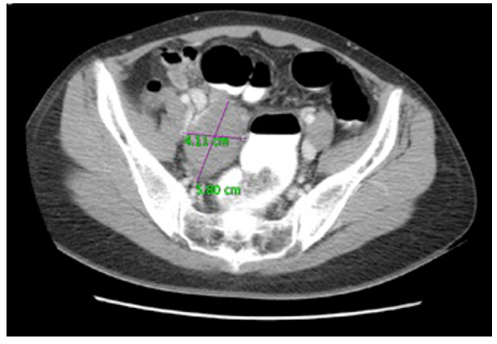
Fig. 2 Abdomen-pelvis computed tomography.

Fig. 3 Right ovarian tumor: operating finding.
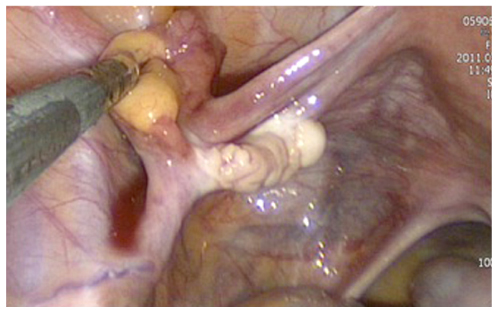
Fig. 4 Left ovarian nodules: operating finding.
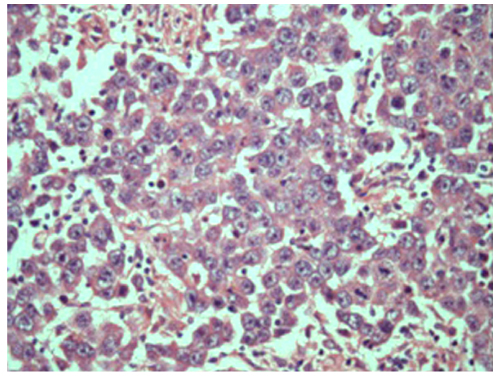
Fig. 5 Right ovarian dysgerminoma pathologic finding (H&E, ×400).
Reference
-
1. Rosen GF, Kaplan B, Lobo RA. Menstrual function and hirsutism in patients with gonadal dysgenesis. Obstet Gynecol. 1988. 71:677–680.2. Donahoe PK, Crawford JD, Hendren WH. Mixed gonadal dysgenesis, pathogensis, and management. J Pediatr Surg. 1979. 14:287–300.3. Tangjitgamol S, Hanprasertpong J, Manusirivithaya S, Wootipoom V, Thavaramara T, Buhachat R. Malignant ovarian germ cell tumors: clinico-pathological presentation and survival outcomes. Acta Obstet Gynecol Scand. 2010. 89:182–189.4. Zalel Y, Piura B, Elchalal U, Czernobilsky B, Antebi S, Dgani R. Diagnosis and management of malignant germ cell ovarian tumors in young females. Int J Gynaecol Obstet. 1996. 55:1–10.5. Troche V, Hernandez E. Neoplasia arising in dysgenetic gonads. Obstet Gynecol Surv. 1986. 41:74–79.6. Sinisi AA, Perrone L, Quarto C, Barone M, Bellastella A, Faggiano M. Dysgerminoma in 45,X Turner syndrome: report of a case. Clin Endocrinol (Oxf). 1988. 28:187–193.7. Olsen MM, Caldamone AA, Jackson CL, Zinn A. Gonadoblastoma in infancy: indications for early gonadectomy in 46XY gonadal dysgenesis. J Pediatr Surg. 1988. 23:270–271.8. Page DC. Hypothesis: a Y-chromosomal gene causes gonadoblastoma in dysgenetic gonads. Development. 1987. 101:Suppl. 151–155.9. Maeyama M, Kagami T, Miyakawa I, Tooya T, Kawasaki N, Iwamasa T. Case report of dysgerminoma in a patient with 46,XX pure gonadal dysgenesis. Gynecol Oncol. 1983. 16:405–413.10. Letterie GS, Page DC. Dysgerminoma and gonadal dysgenesis in a 46,XX female with no evidence of Y chromosomal DNA. Gynecol Oncol. 1995. 57:423–425.11. Plattner G, Oxorn H. Familial incidence of ovarian dermoid cysts. Can Med Assoc J. 1973. 108:892–893.12. Linder D, Hecht F, McCaw BK, Campbell JR. Origin of extragonadal teratomas and endodermal sinus tumours. Nature. 1975. 254:597–598.13. Rayburn WF, Barr M Jr. Teratomas: concordance in mother and fetus. Am J Obstet Gynecol. 1982. 144:110–112.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Dysgerminoma Associated with 46, XY Pure Gonadal Dysgenesis
- A Case of 45 , X/46 , XY Mixed Gonadal Dysgenesis Associated with Azoospermia
- Gonadoblastoma and dysgerminoma associated with 46,XY pure gonadal dysgenesis--a case report
- Gonadoblastoma Overgrown by Dysgerminoma in Women with 46,XX Karyotype: A Report of Two Cases
- Swyer Syndrome: A Case Report
