Optimal Cardiac Magnetic Resonance Contrast-Enhanced Timing Robust Angiography (CMR-CENTRA) for the Three-Dimensional Reconstruction of the Bilateral Atria in the Electroanatomic Mapping (EAM) of Atrial Fibrillation
- Affiliations
-
- 1Department of Radiology, Korea University Anam Hospital, Seoul, Korea. sungho.hwng@gmail.com
- 2Division of Cardiology, Department of Internal Medicine, Korea University Anam Hospital, Seoul, Korea.
- KMID: 2392683
- DOI: http://doi.org/10.13104/imri.2017.21.3.131
Abstract
- PURPOSE
To optimize the timing of scans using cardiac magnetic resonance contrast-enhanced timing robust angiography (CMR-CENTRA) for electroanatomic mapping (EAM) of the right atrium (RA) and left atrium (LA) in patients with atrial fibrillation (AF).
MATERIALS AND METHODS
Fifty patients with AF (38 men; mean age, 59.6 ± 9.3 years) underwent CMR-CENTRA in preparation for EAM. The CMR-CENTRA data were acquired at five different scan times: 0 seconds, 5 seconds, 10 seconds, 15 seconds, and 20 seconds after an intravenous injection of contrast media. To evaluate the degree of contrast enhancement, right atrial relative contrast (RA-RC) and left atrial relative contrast (LA-RC) on the CMR-CENTRA scans were assessed at each time point. The three-dimensional (3D) reconstruction of the RA and LA for the EAM system was performed using the CMR-CENTRA data.
RESULTS
A CMR-CENTRA at a scan time of 10 seconds showed significantly greater LA-RC (P < 0.05) compared with all other scan times. A CMR-CENTRA at a scan time of 15 seconds showed significantly greater RA-RC (P < 0.05) compared with all other scan times. In the 3D reconstruction of the RA, the success rates of CMR-CENTRA at scan times of 10 seconds and 15 seconds were 18% and 100%, respectively. In the 3D reconstruction of the LA, the success rates of CMR-CENTRA at 10- and 15-second scan times were 100%.
CONCLUSION
The CMR-CENTRA data acquired at 15 seconds after the injection of contrast media is appropriate for the preparation of an EAM system that is focused on the RA and LA in patients with AF.
Keyword
MeSH Terms
Figure
-

Fig. 1 Sequential CMR-CENTRA images for the visualization of the contrast media passing through the heart. Coronal images (a) of CMR-CENTRA at 0s, 5s, 10s, 15s, and 20s show the dynamics of contrast media in the left atrium (white arrows). In addition, coronal images of CMR-CENTRA (b) at 0s, 5s, 10s, 15s, and 20s show the dynamics of contrast media in the right atrium. The CMR-CENTRA at 15s shows the weak but homogeneous contrast enhancement in the right atrium as well as the superior vena cava. CMR-CENTRA = cardiac magnetic resonance contrast-enhanced timing robust angiography; LA-RC = left atrial relative contrast; RA-RC = right atrial relative contrast
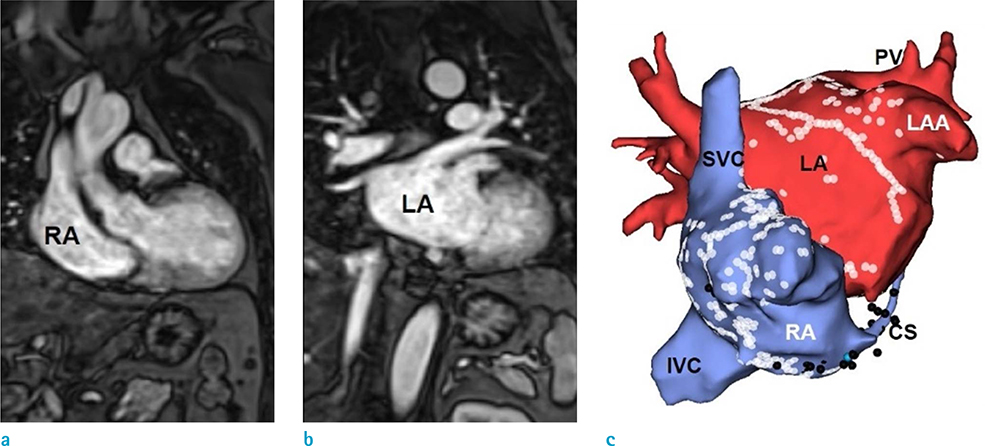
Fig. 2 3D-reconstruction of the right atrium (RA) and left atrium (LA) by using cardiac magnetic resonance contrast-enhanced timing robust angiography (CMR-CENTRA) data acquired at 15s. The 3D-recontstruction of RA and LA from CMR-CENTRA (a, b) provides the ideal RA and LA models (c). Ideal RA model (c) shows the superior vena cava (SVC), inferior vena cava (IVC), coronary sinus (CS), and RA clearly. Ideal LA model (c) shows the pulmonary vein (PV), left atrial appendage (LAA), and LA clearly.
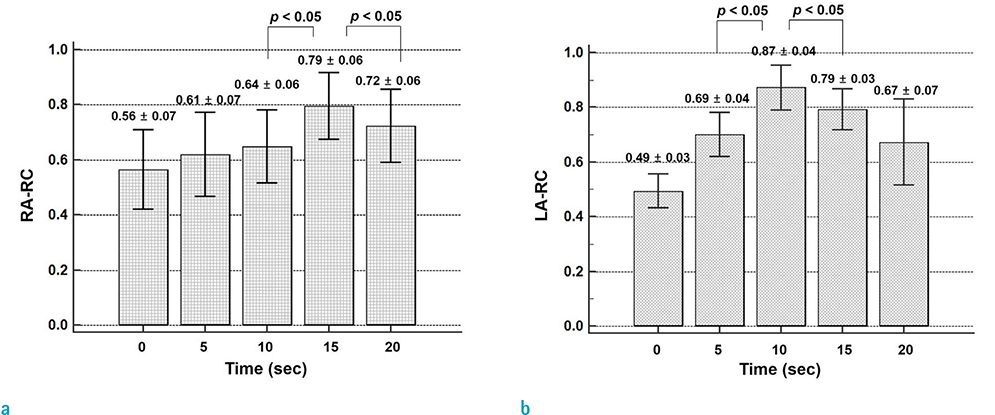
Fig. 3 Comparison of the right atrial relative contrast (RA-RC) (a) and left atrial relative contrast (LA-RC) (b) among the five different scan times of cardiac magnetic resonance contrast-enhanced timing robust angiography (CMR-CENTRA).

Fig. 4 Comparison of the right atrial relative contrast (RA-RC) (a) and left atrial relative contrast (LA-RC) (b) between the ideal and imperfect models of the right atrium (RA) and left atrium (LA).
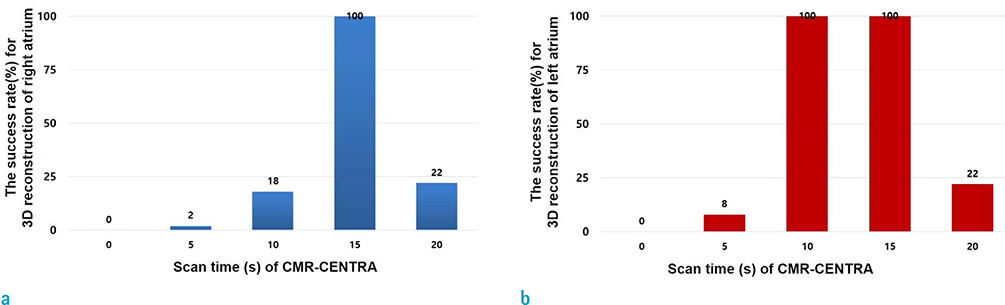
Fig. 5 The success rates for the 3D reconstruction of the right atrium (a) and left atrium (b) using cardiac magnetic resonance contrast-enhanced timing robust angiography (CMR-CENTRA).
Cited by 1 articles
-
Use of Cardiac Computed Tomography and Magnetic Resonance Imaging in Case Management of Atrial Fibrillation with Catheter Ablation
Hee-Gone Lee, Jaemin Shim, Jong-il Choi, Young-Hoon Kim, Yu-Whan Oh, Sung Ho Hwang
Korean J Radiol. 2019;20(5):695-708. doi: 10.3348/kjr.2018.0774.
Reference
-
1. Fuster V, Ryden LE, Cannom DS, et al. ACC/AHA/ESC 2006 Guidelines for the Management of Patients with Atrial Fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation): developed in collaboration with the European Heart Rhythm Association and the Heart Rhythm Society. Circulation. 2006; 114:e257–e354.2. European Heart Rhythm Association. Heart Rhythm Society. Fuster V, et al. ACC/AHA/ESC 2006 guidelines for the management of patients with atrial fibrillation--executive summary: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines and the European Society of Cardiology Committee for Practice Guidelines (Writing Committee to Revise the 2001 Guidelines for the Management of Patients With Atrial Fibrillation). J Am Coll Cardiol. 2006; 48:854–906.3. Haissaguerre M, Sanders P, Hocini M, et al. Catheter ablation of long-lasting persistent atrial fibrillation: critical structures for termination. J Cardiovasc Electrophysiol. 2005; 16:1125–1137.4. Oral H, Chugh A, Yoshida K, et al. A randomized assessment of the incremental role of ablation of complex fractionated atrial electrograms after antral pulmonary vein isolation for long-lasting persistent atrial fibrillation. J Am Coll Cardiol. 2009; 53:782–789.5. Nademanee K, McKenzie J, Kosar E, et al. A new approach for catheter ablation of atrial fibrillation: mapping of the electrophysiologic substrate. J Am Coll Cardiol. 2004; 43:2044–2053.6. Hwang SH, Oh YW, Lee DI, Shim J, Park SW, Kim YH. Relation between left atrial wall composition by late gadolinium enhancement and complex fractionated atrial electrograms in patients with persistent atrial fibrillation: influence of non-fibrotic substrate in the left atrium. Int J Cardiovasc Imaging. 2015; 31:1191–1199.7. Dabir D, Naehle CP, Clauberg R, Gieseke J, Schild HH, Thomas D. High-resolution motion compensated MRA in patients with congenital heart disease using extracellular contrast agent at 3 Tesla. J Cardiovasc Magn Reson. 2012; 14:75.8. Schonberger M, Usman A, Galizia M, Popescu A, Collins J, Carr JC. Time-resolved MR venography of the pulmonary veins precatheter-based ablation for atrial fibrillation. J Magn Reson Imaging. 2013; 37:127–137.9. Yoon YE, Hong YJ, Kim HK, et al. 2014 Korean guidelines for appropriate utilization of cardiovascular magnetic resonance imaging: a joint report of the Korean Society of Cardiology and the Korean Society of Radiology. Korean J Radiol. 2014; 15:659–688.10. Heist EK, Chevalier J, Holmvang G, et al. Factors affecting error in integration of electroanatomic mapping with CT and MR imaging during catheter ablation of atrial fibrillation. J Interv Card Electrophysiol. 2006; 17:21–27.11. Bertaglia E, Brandolino G, Zoppo F, Zerbo F, Pascotto P. Integration of three-dimensional left atrial magnetic resonance images into a real-time electroanatomic mapping system: validation of a registration method. Pacing Clin Electrophysiol. 2008; 31:273–282.12. Jeong HJ, Vakil P, Sheehan JJ, et al. Time-resolved magnetic resonance angiography: evaluation of intrapulmonary circulation parameters in pulmonary arterial hypertension. J Magn Reson Imaging. 2011; 33:225–231.13. Shrout PE, Fleiss JL. Intraclass correlations: uses in assessing rater reliability. Psychol Bull. 1979; 86:420–428.14. Giesel FL, Runge V, Kirchin M, et al. Three-dimensional multiphase time-resolved low-dose contrast-enhanced magnetic resonance angiography using TWIST on a 32-channel coil at 3 T: a quantitative and qualitative comparison of a conventional gadolinium chelate with a high-relaxivity agent. J Comput Assist Tomogr. 2010; 34:678–683.15. Malik SB, Kwan D, Shah AB, Hsu JY. The right atrium: gateway to the heart--anatomic and pathologic imaging findings. Radiographics. 2015; 35:14–31.16. Callan P, Clark AL. Right heart catheterisation: indications and interpretation. Heart. 2016; 102:147–157.17. Hwang SH, Oh YW. Assessment of cor triatriatum dexter and giant eustachian valve with cardiac magnetic resonance. Circulation. 2014; 130:1727–1729.18. Ho SY, Sanchez-Quintana D, Cabrera JA, Anderson RH. Anatomy of the left atrium: implications for radiofrequency ablation of atrial fibrillation. J Cardiovasc Electrophysiol. 1999; 10:1525–1533.19. Lacomis JM, Wigginton W, Fuhrman C, Schwartzman D, Armfield DR, Pealer KM. Multi-detector row CT of the left atrium and pulmonary veins before radio-frequency catheter ablation for atrial fibrillation. Radiographics. 2003; 23(Spec No):S35–S48. discussion S48-50.20. Groarke JD, Waller AH, Vita TS, et al. Feasibility study of electrocardiographic and respiratory gated, gadolinium enhanced magnetic resonance angiography of pulmonary veins and the impact of heart rate and rhythm on study quality. J Cardiovasc Magn Reson. 2014; 16:43.21. Hwang SH, Roh SY, Shim J, Choi JI, Kim YH, Oh YW. Atrial fibrillation: relationship between left atrial pressure and left atrial appendage emptying determined with velocityencoded cardiac MR imaging. Radiology. 2017; 284:381–389.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Advanced Cardiac MR Imaging for Myocardial Characterization and Quantification: T1 Mapping
- Recent Progress of Cardiac MRI for Nuclear Medicine Professionals
- CMR Parametric Mapping as a Tool for Myocardial Tissue Characterization
- Paradoxical Response of Giant Left Atrial Appendage Aneurysm after Catheter Ablation of Atrial Fibrillation
- Drug Therapy and Catheter Ablation for Atrial Fibrillation
