Ultrasonographic Features of Complications Associated with Injectable Fillers in the Cervicofacial Region
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea. hshong@schmc.ac.kr
- 2Department of Pathology, Soonchunhyang University College of Medicine, Bucheon Hospital, Bucheon, Korea.
- KMID: 2392118
- DOI: http://doi.org/10.3348/jksr.2017.77.4.222
Abstract
- PURPOSE
The aim of this study was to evaluate the ultrasonographic (US) features of complications associated with injectable fillers in the cervicofacial region.
MATERIALS AND METHODS
This retrospective study was approved by our Institutional Review Board. Thirty-nine patients (37 females and 2 males; mean age: 52 years; age range: 26-83 years), both symptomatic (n = 32) and asymptomatic (n = 7), who underwent cosmetic procedures in the cervicofacial area and US, were included.
RESULTS
All of the cases were classified into five types based on major US features, including (the most common feature) diffuse high echogenicity with posterior snow storming (n = 17, 39%). The other types included a hypoechoic nodule with high echoic lines (n = 10, 23%), a round hypoechoic nodule (n = 12, 27%), a heterogeneously echogenic lesion with internal echoic dots (n = 1, 2%) and an ill-defined non-mass-like fatty lesion (n = 4, 9%). The time between cosmetic injection and evaluation was variable (range: 3 weeks-21 years). Usually, the injected material was either unknown or illegal (n = 24). Ten patients underwent pathological evaluation. Many histological types of foreign body granulomas were evident.
CONCLUSION
Knowledge of the US features of complications associated with fillers may reduce the likelihood of misinterpreting the injected area as a true lesion, in turn decreasing unnecessary invasive procedures and costs for patients.
MeSH Terms
Figure
-
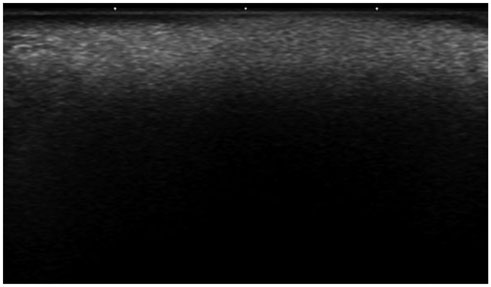
Fig. 1 A 57-year-old woman underwent US for evaluation of migration of nodules in the forehead and the nasal root. She had a history of illegal injections into the forehead, nose, both nasolabial folds and chin. Transverse US scan of the chin reveals diffuse high echogenicity with posterior snow storming (type 1).
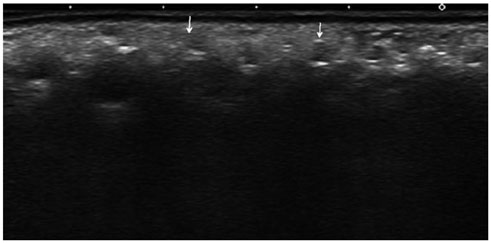
Fig. 2 A 51-year-old woman had a history of illegal filler injection into her cheeks, chin, and forehead 8 years earlier. She complained of migration of the injected materials and a palpable mass in her right cheek. A transverse US scan reveals a hypoechoic nodule with anterior and posterior high echoic lines (type 2, arrows).

Fig. 3 A 66-year-old woman had a history of collagen injection into the forehead, both glabellae, nasolabial folds, and the upper lip 4 years earlier. She underwent US because of a palpable mass in the forehead. A. A transverse scan of the forehead reveals a round hypoechoic nodule (type 3). B. Angulated foreign materials with multinucleated giant cells and an asteroid body are observed (hematoxylin and eosin staining, × 200). C. The foreign materials are negative for Alcian blue staining (× 200).
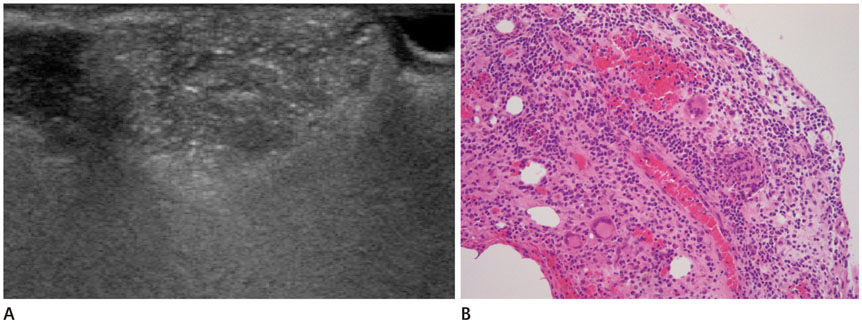
Fig. 4 A 49-year-old woman complained of a palpable mass in nasolabial folds of 1–2 months duration. She had been injected with collagen and steroid. A. A transverse US scan reveals an heterogeneously hyperechoic lesion with internal echoic dots (type 4). B. Biopsy reveals both acute and chronic inflammation and several multinucleated giant cells (hematoxylin and eosin staining, × 200).
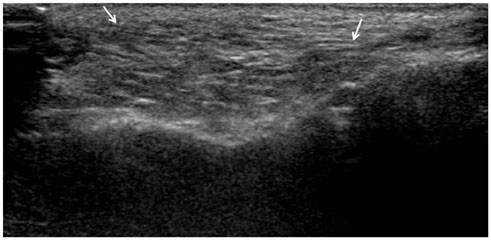
Fig. 5 A 33-year-old woman complained of a palpable mass beneath the lower eyelid. She had a history of autologous fat injection at the same site 9 months earlier. US shows an ill-defined, nonmass-like fatty lesion (type 5, arrows).
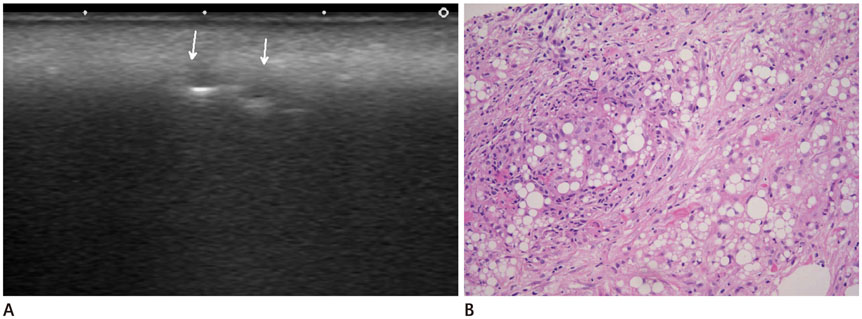
Fig. 6 An 83-year-old woman underwent US for evaluation of an erythematous swelling in the anterior neck and the submandibular space. She had a history of illegal injections into the face and neck to smoothen wrinkles 5 years earlier. She did not initially disclose her previous history of an esthetic procedure. During US, she confirmed her history, and a biopsy was performed. A. Transverse US of the neck reveals high echogenicity with posterior snow storming (type 1) throughout the subcutaneous fatty layer, and a low echoic nodule with a peripheral hyperechoic rim and posterior enhancement (type 2, arrows). B. The US-guided gun biopsy specimen shows various vacuoles associated with chronic inflammation, fibrosis, and ill-defined granulomas (hematoxylin and eosin staining, × 100).
Reference
-
1. Kontis TC, Rivkin A. The history of injectable facial fillers. Facial Plast Surg. 2009; 25:67–72.2. Goldberg DJ. Breakthroughs in US dermal fillers for facial soft-tissue augmentation. J Cosmet Laser Ther. 2009; 11:240–247.3. Ginat DT, Schatz CJ. Imaging features of midface injectable fillers and associated complications. AJNR Am J Neuroradiol. 2013; 34:1488–1495.4. Christensen L, Breiting V, Janssen M, Vuust J, Hogdall E. Adverse reactions to injectable soft tissue permanent fillers. Aesthetic Plast Surg. 2005; 29:34–48.5. Lombardi T, Samson J, Plantier F, Husson C, Küffer R. Orofacial granulomas after injection of cosmetic fillers. Histopathologic and clinical study of 11 cases. J Oral Pathol Med. 2004; 33:115–120.6. Dayan SH, Bassichis BA. Facial dermal fillers: selection of appropriate products and techniques. Aesthet Surg J. 2008; 28:335–347.7. Jham BC, Nikitakis NG, Scheper MA, Papadimitriou JC, Levy BA, Rivera H. Granulomatous foreign-body reaction involving oral and perioral tissues after injection of biomaterials: a series of 7 cases and review of the literature. J Oral Maxillofac Surg. 2009; 67:280–285.8. Wortsman X, Wortsman J, Orlandi C, Cardenas G, Sazunic I, Jemec GB. Ultrasound detection and identification of cosmetic fillers in the skin. J Eur Acad Dermatol Venereol. 2012; 26:292–301.9. Young SR, Bolton PA, Downie J. Use of high-frequency ultrasound in the assessment of injectable dermal fillers. Skin Res Technol. 2008; 14:320–323.10. Mastruserio DN, Pesqueira MJ, Cobb MW. Severe granulomatous reaction and facial ulceration occurring after subcutaneous silicone injection. J Am Acad Dermatol. 1996; 34(5 Pt 1):849–852.11. Maly A, Regev E, Meir K, Maly B. Tissue reaction to liquid silicone simulating low-grade liposarcoma following lip augmentation. J Oral Pathol Med. 2004; 33:314.12. Morhenn VB, Lemperle G, Gallo RL. Phagocytosis of different particulate dermal filler substances by human macrophages and skin cells. Dermatol Surg. 2002; 28:484–490.13. Shafir R, Amir A, Gur E. Long-term complications of facial injections with Restylane (injectable hyaluronic acid). Plast Reconstr Surg. 2000; 106:1215–1216.14. Requena C, Izquierdo MJ, Navarro M, Martínez A, Vilata JJ, Botella R, et al. Adverse reactions to injectable aesthetic microimplants. Am J Dermatopathol. 2001; 23:197–202.15. Verpaele A, Strand A. Restylane SubQ, a non-animal stabilized hyaluronic acid gel for soft tissue augmentation of the mid- and lower face. Aesthet Surg J. 2006; 26:S10–S17.16. Reda-Lari A. Augmentation of the malar area with polyacrylamide hydrogel: experience with more than 1300 patients. Aesthet Surg J. 2008; 28:131–138.17. Sturm LP, Cooter RD, Mutimer KL, Graham JC, Maddern GJ. A systematic review of dermal fillers for age-related lines and wrinkles. ANZ J Surg. 2011; 81:9–17.18. Judodihardjo H, Dykes P. Objective and subjective measurements of cutaneous inflammation after a novel hyaluronic acid injection. Dermatol Surg. 2008; 34:Suppl 1. S110–S114.19. Lemperle G, Gauthier-Hazan N, Wolters M, Eisemann-Klein M, Zimmermann U, Duffy DM. Foreign body granulomas after all injectable dermal fillers: part 1. Possible causes. Plast Reconstr Surg. 2009; 123:1842–1863.20. Lemperle G, Rullan PP, Gauthier-Hazan N. Avoiding and treating dermal filler complications. Plast Reconstr Surg. 2006; 118:3 Suppl. 92S–107S.21. Baumann LS, Halem ML. Lip silicone granulomatous foreign body reaction treated with aldara (imiquimod 5%). Dermatol Surg. 2003; 29:429–443.22. Rapaport MJ, Vinnik C, Zarem H. Injectable silicone: cause of facial nodules, cellulitis, ulceration, and migration. Aesthetic Plast Surg. 1996; 20:267–276.23. Hirsch RJ, Stier M. Complications of soft tissue augmentation. J Drugs Dermatol. 2008; 7:841–845.24. Schelke LW, Van Den Elzen HJ, Erkamp PP, Neumann HA. Use of ultrasound to provide overall information on facial fillers and surrounding tissue. Dermatol Surg. 2010; 36:Suppl 3. 1843–1851.25. Wortsman X, Wortsman J. Clinical usefulness of variable-frequency ultrasound in localized lesions of the skin. J Am Acad Dermatol. 2010; 62:247–256.26. Kuwano Y, Ishizaki K, Watanabe R, Nanko H. Efficacy of diagnostic ultrasonography of lipomas, epidermal cysts, and ganglions. Arch Dermatol. 2009; 145:761–764.27. Fischer J, Metzler G, Schaller M. Cosmetic permanent fillers for soft tissue augmentation: a new contraindication for interferon therapies. Arch Dermatol. 2007; 143:507–510.28. Feeney JN, Fox JJ, Akhurst T. Radiological impact of the use of calcium hydroxylapatite dermal fillers. Clin Radiol. 2009; 64:897–902.29. Requena L, Requena C, Christensen L, Zimmermann US, Kutzner H, Cerroni L. Adverse reactions to injectable soft tissue fillers. J Am Acad Dermatol. 2011; 64:1–34. quiz 35-36.30. Dadzie OE, Mahalingam M, Parada M, El Helou T, Philips T, Bhawan J. Adverse cutaneous reactions to soft tissue fillers--a review of the histological features. J Cutan Pathol. 2008; 35:536–548.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A revision and summary of injectable fillers
- Management of a Visible Nodule Following Poly-L-Lactic Acid Injection in the Periorbital Area
- Long-Term Side Effects of Soft Tissue Filler Injection
- Remote migration of breast filler to the inguinal area: a case report
- Late-Onset Complication of Fillers: Paraffinoma of the Lower Eyelids Clinically Mimicking Xanthelasma
