Submillisievert Computed Tomography of the Chest in Contact Investigation for Drug-Resistant Tuberculosis
- Affiliations
-
- 1Division of HIV and Tuberculosis Control, Korea Centers for Disease Control and Prevention, Seoul, Korea.
- 2Department of Radiology, Seoul National University College of Medicine, Seoul, Korea. jmgoo@plaza.snu.ac.kr
- 3Institute of Radiation Medicine, Seoul National University Medical Research Center, Seoul, Korea.
- 4Division of Pulmonary and Critical Care Medicine, Department of Internal Medicine, Seoul National University College of Medicine, Seoul, Korea.
- 5Korean Institute of Tuberculosis, Seoul, Korea.
- KMID: 2390303
- DOI: http://doi.org/10.3346/jkms.2017.32.11.1779
Abstract
- Close contacts with infectious tuberculosis (TB) are persons at high risk for developing active disease. We preliminarily introduced submillisievert chest computed tomography (CT) scan (effective dose, 0.19-0.25 millisievert) in a contact investigation of multi-drug resistant (MDR)-TB. Baseline CT scan showed minimal nodules or branching opacities in two of six contacts. A two-month follow-up examination revealed a radiologic progression in contact 1, subsequently having the microbiologic diagnosis of MDR-TB at an asymptomatic early stage, whereas nodules transiently increased after 3 months in contact 2, followed by a decrease after one year. Contact 1 was cured after 1.5-year of anti-MDR-TB treatment. In conclusion, early identification of secondary MDR-TB is feasible with submillisievert chest CT scans in contact investigations of MDR-TB, minimizing of MDR-TB transmission and offering a favorable treatment outcome. This was a clinical trial study and was registered at www.ClinicalTrials.gov (Identifier: NCT02454738).
Keyword
MeSH Terms
Figure
-

Fig. 1 Chest radiograph and CT of a secondary case of MDR-TB in contact 1. (A) Chest radiograph at baseline contact investigation is normal. (B) Baseline submillisievert computed tomographic scans of the chest shows tuberculous granuloma and focal bronchiolitis (arrows) in the superior segment of the right lower lobe on baseline scan. (C) Chest radiograph 2 months later shows subtle opacities (arrow) in the right upper lung zone. (D) Submillisievert computed tomographic scans of the chest 2 months later shows the progression of pre-existing lesions into ill-defined lobular consolidation (arrows) in the superior segment of the right lower lobe. (E) Results of spoligotyping 24-loci MIRU-VNTR analysis are identical between index and secondary MDR-TB. (F) Chest radiograph taken after completion of 1.5-year of anti-MDR-TB treatment shows small residual opacity (arrows) in the right upper lung zone. CT = computed tomography, MDR-TB = multi-drug resistant tuberculosis, MIRU-VNTR = mycobacterial interspersed repetitive units-variable-number tandem repeats, TB = tuberculosis.
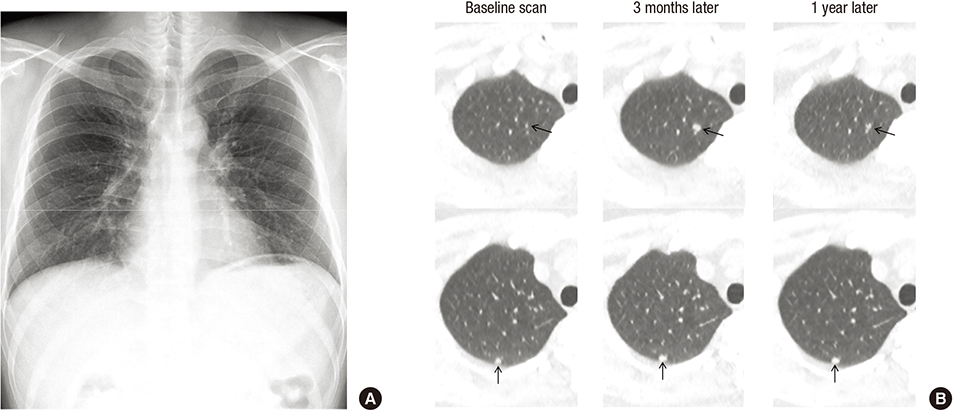
Fig. 2 Chest radiograph and CT in contact 2, having sub-centimeter-sized nodules. (A) Chest radiograph at baseline contact investigation is normal. (B) Baseline, 3-month, and 1-year follow-up submillisievert computed tomographic scans of the chest shows two suspected tuberculous granulomas (arrows). Lesions increased slightly 3 months later, and decreased after 1 year of observation. CT = computed tomography.
Reference
-
1. World Health Organization. Global tuberculosis report 2015 [Internet]. accessed on 29 August 2017. Available at http://apps.who.int/iris/bitstream/10665/191102/1/9789241565059_eng.pdf.2. Kim HJ, Yoon HH, Eun BW, Ahn Y, Ryoo S, Kim HJ. The rate of drug-resistant tuberculosis in Korean children and adolescents since 2007. J Korean Med Sci. 2017; 32:954–960.3. Gandhi NR, Nunn P, Dheda K, Schaaf HS, Zignol M, van Soolingen D, Jensen P, Bayona J. Multidrug-resistant and extensively drug-resistant tuberculosis: a threat to global control of tuberculosis. Lancet. 2010; 375:1830–1843.4. Shah NS, Yuen CM, Heo M, Tolman AW, Becerra MC. Yield of contact investigations in households of patients with drug-resistant tuberculosis: systematic review and meta-analysis. Clin Infect Dis. 2014; 58:381–391.5. Becerra MC, Appleton SC, Franke MF, Chalco K, Arteaga F, Bayona J, Murray M, Atwood SS, Mitnick CD. Tuberculosis burden in households of patients with multidrug-resistant and extensively drug-resistant tuberculosis: a retrospective cohort study. Lancet. 2011; 377:147–152.6. van der Werf MJ, Langendam MW, Sandgren A, Manissero D. Lack of evidence to support policy development for management of contacts of multidrug-resistant tuberculosis patients: two systematic reviews. Int J Tuberc Lung Dis. 2012; 16:288–296.7. Langendam MW, Tiemersma EW, van der Werf MJ, Sandgren A. Adverse events in healthy individuals and MDR-TB contacts treated with anti-tuberculosis drugs potentially effective for preventing development of MDR-TB: a systematic review. PLoS One. 2013; 8:e53599.8. Falzon D, Jaramillo E, Schünemann HJ, Arentz M, Bauer M, Bayona J, Blanc L, Caminero JA, Daley CL, Duncombe C, et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur Respir J. 2011; 38:516–528.9. Barry CE 3rd, Boshoff HI, Dartois V, Dick T, Ehrt S, Flynn J, Schnappinger D, Wilkinson RJ, Young D. The spectrum of latent tuberculosis: rethinking the biology and intervention strategies. Nat Rev Microbiol. 2009; 7:845–855.10. Lee SW, Jang YS, Park CM, Kang HY, Koh WJ, Yim JJ, Jeon K. The role of chest CT scanning in TB outbreak investigation. Chest. 2010; 137:1057–1064.11. Petruccioli E, Scriba TJ, Petrone L, Hatherill M, Cirillo DM, Joosten SA, Ottenhoff TH, Denkinger CM, Goletti D. Correlates of tuberculosis risk: predictive biomarkers for progression to active tuberculosis. Eur Respir J. 2016; 48:1751–1763.12. Alsdurf H, Hill PC, Matteelli A, Getahun H, Menzies D. The cascade of care in diagnosis and treatment of latent tuberculosis infection: a systematic review and meta-analysis. Lancet Infect Dis. 2016; 16:1269–1278.13. Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med. 2007; 357:2277–2284.14. Deak PD, Smal Y, Kalender WA. Multisection CT protocols: sex- and age-specific conversion factors used to determine effective dose from dose-length product. Radiology. 2010; 257:158–166.15. Pearce MS, Salotti JA, Little MP, McHugh K, Lee C, Kim KP, Howe NL, Ronckers CM, Rajaraman P, Sir Craft AW, et al. Radiation exposure from CT scans in childhood and subsequent risk of leukaemia and brain tumours: a retrospective cohort study. Lancet. 2012; 380:499–505.16. Mettler FA Jr, Huda W, Yoshizumi TT, Mahesh M. Effective doses in radiology and diagnostic nuclear medicine: a catalog. Radiology. 2008; 248:254–263.17. Lenaerts A, Barry CE 3rd, Dartois V. Heterogeneity in tuberculosis pathology, microenvironments and therapeutic responses. Immunol Rev. 2015; 264:288–307.18. Im JG, Itoh H, Shim YS, Lee JH, Ahn J, Han MC, Noma S. Pulmonary tuberculosis: CT findings--early active disease and sequential change with antituberculous therapy. Radiology. 1993; 186:653–660.19. Yoon CG, Oh SY, Lee JB, Kim MH, Seo Y, Yang J, Bae KJ, Hong S, Yang ES, Kim HJ. Occupational risk of latent tuberculosis infection in health workers of 14 military hospitals. J Korean Med Sci. 2017; 32:1251–1257.20. de Visser V, Sotgiu G, Lange C, Aabye MG, Bakker M, Bartalesi F, Brat K, Chee CB, Dheda K, Dominguez J, et al. False-negative interferon-γ release assay results in active tuberculosis: a TBNET study. Eur Respir J. 2015; 45:279–283.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Evolution of Interferon-Gamma Release Assay Results and Submillisievert Chest CT Findings among Close Contacts of Active Pulmonary Tuberculosis Patients
- Diagnosis of Pulmonary Tuberculosis: Recent Advances and Diagnostic Algorithms
- Multidrug-resistant Pulmonary Tuberculosis Among Young Korean Soldiers in a Communal Setting
- Medical Management of Drug-Resistant Tuberculosis
- Drug-Resistant Pulmonary Tuberculosis in Kosin Medical Center
