Dentinogenesis imperfecta type II: A case report with 17 years of follow-up
- Affiliations
-
- 1Department of Oral Health, School of Dentistry, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Brazil.
- 2Department of Oral Radiology, School of Dentistry, Pontifical Catholic University of Minas Gerais, Belo Horizonte, Brazil. manzi@pucminas.br
- KMID: 2389894
- DOI: http://doi.org/10.5624/isd.2017.47.2.129
Abstract
- Dentinogenesis imperfecta is a dominant autosomal hereditary disorder of dentin formation that affects the deciduous and permanent teeth. Its etiology is characterized by inadequate cell differentiation during odontogenesis. The clinical characteristics of dentinogenesis imperfecta are discolored teeth with a translucency that varies from gray to brown or amber. Radiographically, the teeth exhibit pulp obliteration, thin and short roots, bell-shaped crowns, and periapical bone rarefaction. The aim of this report was to present a case of dentinogenesis imperfecta type II that was followed up over a 17-year period. This report also presents scanning electron microscopy images of the enamel and dentin, showing that both were altered in the affected teeth. The disease characteristics and the treatments that were administered are reported in this study to guide dentists with respect to the need for early diagnosis and adequate follow-up to avoid major sequelae.
MeSH Terms
Figure
-
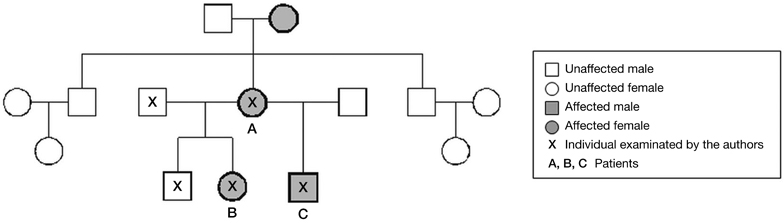
Fig. 1 Pedigree of dentinogenesis imperfecta in the patient's family medical record, covering 3 generations.
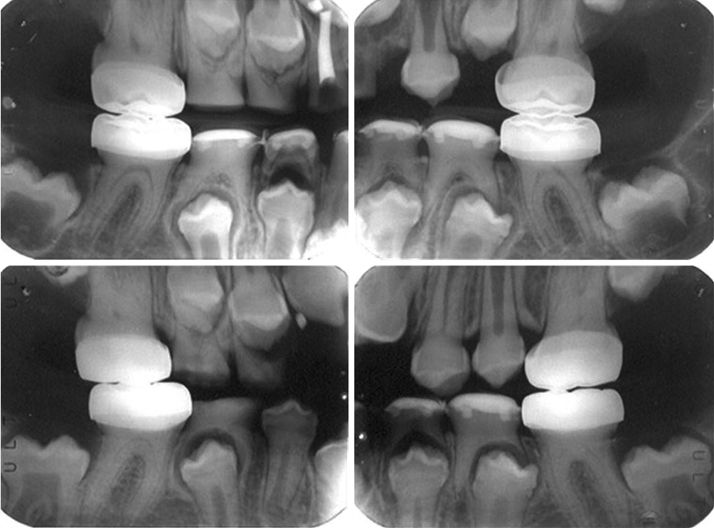
Fig. 2 Radiographic images of the 7-year-old patient. Temporary stainless steel crowns are present in the permanent first molars, and direct composite resin restorations are present in the primary mandibular molars.
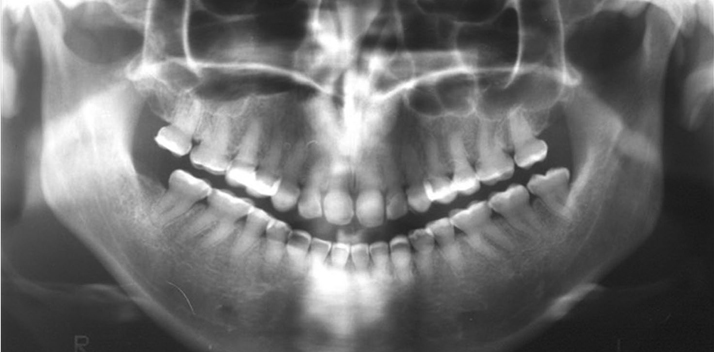
Fig. 3 Panoramic radiograph of the patient at 20 years of age, showing obliterated pulp chambers, shortened crowns restored with resin, and thin roots with constriction in the cervical region.
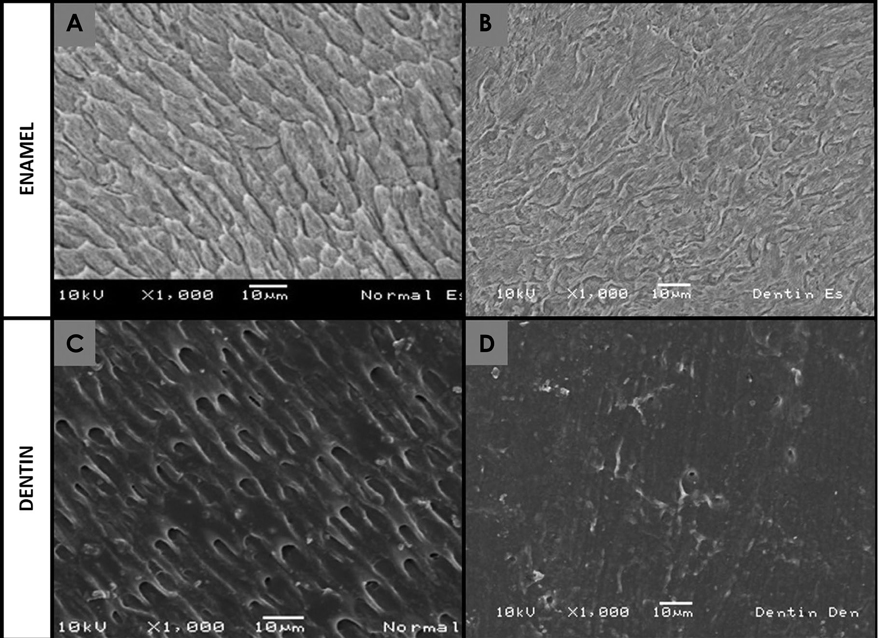
Fig. 4 Scanning electron microscopy images (×1000) show the enamel and dentin of both a normal tooth and a tooth affected by dentinogenesis imperfecta. A. Parallelism of the prismatic enamel crystals can be observed. B. Absence of parallelism in the prismatic enamel crystals is found. C. Normal dentin structure with a tubular direction throughout its entire structure is found. D. Affected dentin structure with the obliteration and reduction of the quantity of dentin tubules is seen.
Reference
-
1. Shields ED, Bixler D, El-Kafrawy AM. A proposed classification for heritable human dentine defects with a description of a new entity. Arch Oral Biol. 1973; 18:543–553.
Article2. MacDougall M, Dong J, Acevedo AC. Molecular basis of human dentin diseases. Am J Med Genet A. 2006; 140:2536–2546.
Article3. Witkop CJ Jr. Amelogenesis imperfecta, dentinogenesis imperfecta and dentin displasia revisted: problems in classification. J Oral Pathol. 1988; 17:547–553.4. Kim JW, Simmer JP. Hereditary dentin defects. J Dent Res. 2007; 86:392–399.
Article5. Witkop CJ Jr. Hereditary defects of dentin. Dent Clin North Am. 1975; 19:25–45.6. Devaraju D, Devi BY, Vasudevan V, Manjunath V. Dentinogenesis imperfecta type I: a case report with literature review on nomenclature system. J Oral Maxillofac Pathol. 2014; 18:Suppl 1. S131–S134.
Article7. Knezević A, Tarle Z, Pandurić V. Esthetic reconstruction of teeth in patient with dentinogenesis imperfecta - a case report. Coll Antropol. 2006; 30:231–234.8. Modesto A, Alves AC, Vieira AR, Portella W. Dentinogenesis imperfecta type II: case report. Braz Dent J. 1996; 7:47–52.9. Ranta H, Lukinmaa PL, Waltimo J. Heritable dentin defects: nosology, pathology, and treatment. Am J Med Genet. 1993; 45:193–200.
Article10. Singh M, Singh S. Hereditary opalescent dentin - a case report. J Indian Soc Pedod Prev Dent. 2004; 22:144–147.11. Koenig MM, Taylor DT. Hereditary opalescent dentin. ASDC J Dent Child. 1973; 40:461–466.12. Wieczorek A, Loster J. Dentinogenesis imperfecta type II: ultrastructure of teeth in sagittal sections. Folia Histochem Cytobiol. 2013; 51:244–247.
Article13. Leal CT, Martins LD, Verli FD, de Souza MA, Ramos-Jorge ML. Case report: clinical, histological and ultrastructural characterization of type II dentinogenesis imperfecta. Eur Arch Paediatr Dent. 2010; 11:306–309.14. Davis GR, Fearne JM, Sabel N, Noren JG. Microscopic study of dental hard tissues in primary teeth with dentinogenesis imperfecta type II: correlation of 3D imaging using X-ray microtomography and polarising microscopy. Arch Oral Biol. 2015; 60:1013–1020.
Article15. Regezi JA, Sciubba JJ, Jordan RC. Oral pathology: clinical pathologic correlations. 7th ed. Philadelphia: Saunders;2017. p. 373–388.16. Gallusi G, Libonati A, Campanella V. SEM-morphology in dentinogenesis imperfecta type II: microscopic anatomy and efficacy of a dentine bonding system. Eur J Paediatr Dent. 2006; 7:9–17.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Blue Sclera in Osteogenesis Imperfecta
- Osteogenesis Imperfecta (Correction of Anterior Tibial Bowing): A case report
- A Case of Neurofibromatosis Type I with Osteogenesis Imperfecta Type I
- A Case of Type I Osteogenesis Imperfecta Differentially Diagnosed as a Cause of a Spinal Compression Fracture
- Full-mouth rehabilitation with CAD/CAM monolithic zirconia in dentinogenesis imperfecta: a case report
