J Endocr Surg.
2017 Sep;17(3):104-113. 10.16956/jes.2017.17.3.104.
Prediction of Transient and Permanent Hypoparathyroidism after Total Thyroidectomy Using the Postoperative Serum Parathyroid Hormone Test: When Is the Best Time to Check?
- Affiliations
-
- 1Department of Surgery, Seoul National University Bundang Hospital, Seongnam, Korea. juneychoi@snubh.org
- 2Department of Surgery, Seoul National University Hospital, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- 4Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 5Department of Surgery, Gachon University Gil Medical Center, Incheon, Korea.
- KMID: 2389590
- DOI: http://doi.org/10.16956/jes.2017.17.3.104
Abstract
- PURPOSE
The usefulness of serum intact parathyroid hormone (iPTH) levels for predicting hypocalcemia after total thyroidectomy is well established. This retrospective cohort study aimed to identify the best time iPTH levels should be checked, and determine the postoperative day 1 iPTH level that most safely predict the development of permanent hypoparathyroidism after total thyroidectomy.
METHODS
All consecutive patients who underwent total thyroidectomy in 2013-2015 were identified, retrospectively. iPTH was measured at 2 hours after thyroidectomy, and on postoperative days 1 and 2, and 12 months after surgery.
RESULTS
In total, 730 patients were included. Their iPTH levels on postoperative day 2 correlated better with postoperative day 1 levels (Pearson's r=0.915) than with iPTH levels at 2 hours after total thyroidectomy (r=0.786). Fourteen patients had normal iPTH levels at 2 hours after thyroidectomy but abnormal levels on postoperative days 1 and 2. On the other hand, 38 patients had abnormal iPTH levels at 2 hours after thyroidectomy but normal values on postoperative days 1 and 2. Receiver operating characteristic analysis showed that the iPTH value of 3.05 pg/mL best predicted permanent hypoparathyroidism (sensitivity, 92.9%; specificity, 99.7%). The safe cutoff value was 9.65 pg/mL (sensitivity, 70.9%; specificity, 100%).
CONCLUSION
A single measurement of iPTH on postoperative day 1 predicted patients at risk of transient hypocalcemia more accurately than measurements at 2 hours after surgery, and thus, can serve widely as a predictor of permanent hypoparathyroidism.
MeSH Terms
Figure
-
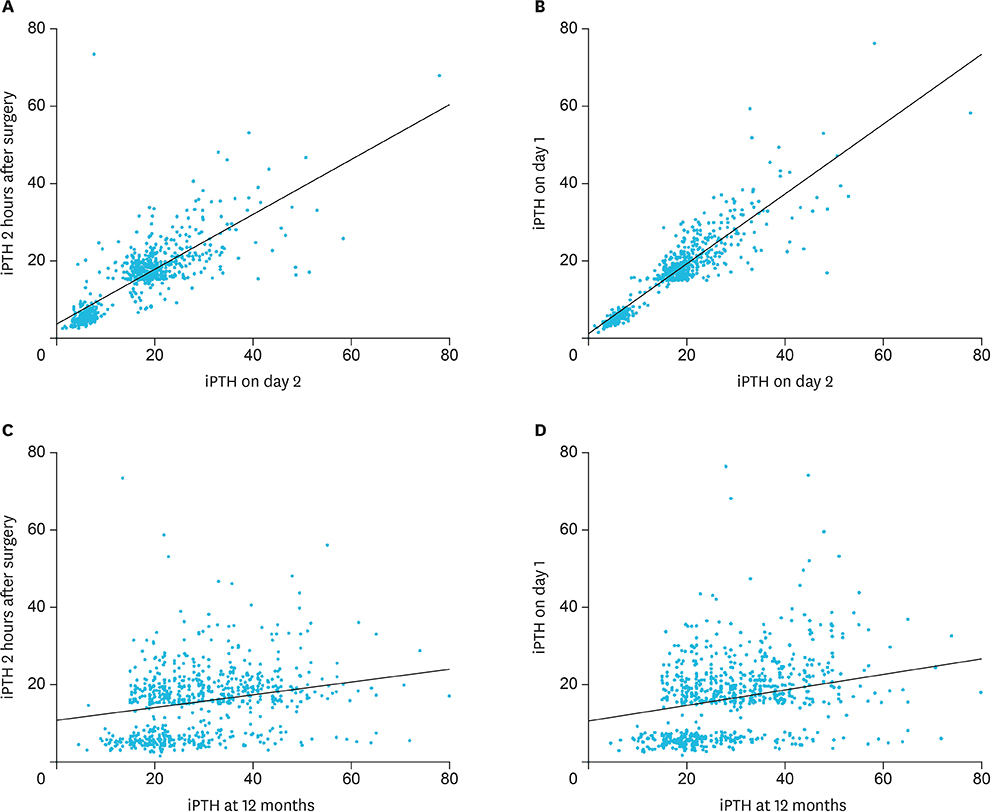
Fig. 1 Correlations between the iPTH levels (A) at 2 hours after surgery and on postoperative days 2 (r=0.786; P<0.001), (B) on days 1 and 2 (r=0.915, P<0.001), (C) at 2 hours after surgery and 12 months (r=0.258; P<0.001), and (D) on day 1 and at 12 months (r=0.277, P<0.001). iPTH = intact parathyroid hormone.
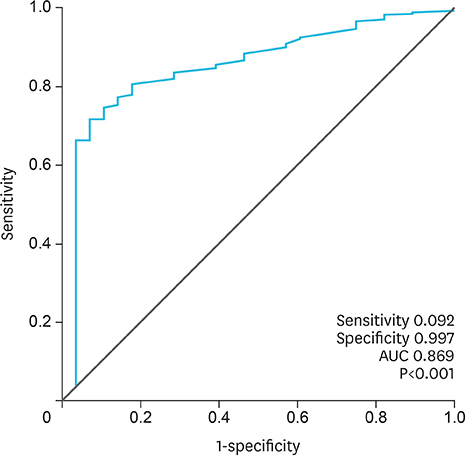
Fig. 2 Performance of day 1 iPTH level analyzed by ROC curve analyses. iPTH = intact parathyroid hormone; ROC = receiver operating characteristic; AUC = area under the curve.
Reference
-
1. Asari R, Passler C, Kaczirek K, Scheuba C, Niederle B. Hypoparathyroidism after total thyroidectomy: a prospective study. Arch Surg. 2008; 143:132–137.2. Warren FM, Andersen PE, Wax MK, Cohen JI. Intraoperative parathyroid hormone levels in thyroid and parathyroid surgery. Laryngoscope. 2002; 112:1866–1870.
Article3. Pattou F, Combemale F, Fabre S, Carnaille B, Decoulx M, Wemeau JL, et al. Hypocalcemia following thyroid surgery: incidence and prediction of outcome. World J Surg. 1998; 22:718–724.
Article4. Raffaelli M, De Crea C, Carrozza C, D'Amato G, Zuppi C, Bellantone R, et al. Combining early postoperative parathyroid hormone and serum calcium levels allows for an efficacious selective post-thyroidectomy supplementation treatment. World J Surg. 2012; 36:1307–1313.
Article5. Sywak MS, Palazzo FF, Yeh M, Wilkinson M, Snook K, Sidhu SB, et al. Parathyroid hormone assay predicts hypocalcaemia after total thyroidectomy. ANZ J Surg. 2007; 77:667–670.
Article6. McLeod IK, Arciero C, Noordzij JP, Stojadinovic A, Peoples G, Melder PC, et al. The use of rapid parathyroid hormone assay in predicting postoperative hypocalcemia after total or completion thyroidectomy. Thyroid. 2006; 16:259–265.
Article7. Vanderlei FA, Vieira JG, Hojaij FC, Cervantes O, Kunii IS, Ohe MN, et al. Parathyroid hormone: an early predictor of symptomatic hypocalcemia after total thyroidectomy. Arq Bras Endocrinol Metabol. 2012; 56:168–172.
Article8. Carr AA, Yen TW, Fareau GG, Cayo AK, Misustin SM, Evans DB, et al. A single parathyroid hormone level obtained 4 hours after total thyroidectomy predicts the need for postoperative calcium supplementation. J Am Coll Surg. 2014; 219:757–764.
Article9. Grodski S, Serpell J. Evidence for the role of perioperative PTH measurement after total thyroidectomy as a predictor of hypocalcemia. World J Surg. 2008; 32:1367–1373.
Article10. McCullough M, Weber C, Leong C, Sharma J. Safety, efficacy, and cost savings of single parathyroid hormone measurement for risk stratification after total thyroidectomy. Am Surg. 2013; 79:768–774.
Article11. Del Río L, Castro A, Bernáldez R, Del Palacio A, Giráldez CV, Lecumberri B, et al. Parathyroid hormone as a predictor of post-thyroidectomy hypocalcemia. Acta Otorrinolaringol Esp. 2011; 62:265–273.
Article12. Lombardi CP, Raffaelli M, Princi P, Santini S, Boscherini M, De Crea C, et al. Early prediction of postthyroidectomy hypocalcemia by one single iPTH measurement. Surgery. 2004; 136:1236–1241.
Article13. AlQahtani A, Parsyan A, Payne R, Tabah R. Parathyroid hormone levels 1 hour after thyroidectomy: an early predictor of postoperative hypocalcemia. Can J Surg. 2014; 57:237–240.
Article14. Cayo AK, Yen TW, Misustin SM, Wall K, Wilson SD, Evans DB, et al. Predicting the need for calcium and calcitriol supplementation after total thyroidectomy: results of a prospective, randomized study. Surgery. 2012; 152:1059–1067.
Article15. AES Guidelines 06/01 Group. Australian Endocrine Surgeons Guidelines AES06/01. Postoperative parathyroid hormone measurement and early discharge after total thyroidectomy: analysis of Australian data and management recommendations. ANZ J Surg. 2007; 77:199–202.16. Choi JY, Lee KE, Youn YK. Bilateral axillo-breast approach(BABA) endoscopic and robotic thyroid surgery. In : Linos D, Chung WY, editors. Minimally Invasive Thyroidectomy. Berlin: Springer;2012. p. 169–182.17. Palestro CJ, Tomas MB, Tronco GG. Radionuclide imaging of the parathyroid glands. Semin Nucl Med. 2005; 35:266–276.
Article18. Khan MI, Waguespack SG, Hu MI. Medical management of postsurgical hypoparathyroidism. Endocr Pract. 2011; 17:Suppl 1. 18–25.
Article19. Rastogi R, Beauchamp NJ, Ladenson PW. Calcification of the basal ganglia in chronic hypoparathyroidism. J Clin Endocrinol Metab. 2003; 88:1476–1477.
Article20. Rajendram R, Deane JA, Barnes M, Swift PG, Adamson K, Pearce S, et al. Rapid onset childhood cataracts leading to the diagnosis of autoimmune polyendocrinopathy-candidiasis-ectodermal dystrophy. Am J Ophthalmol. 2003; 136:951–952.
Article21. Kinirons MJ, Glasgow JF. The chronology of dentinal defects related to medical findings in hypoparathyroidism. J Dent. 1985; 13:346–349.
Article22. Reid IR, Bristow SM, Bolland MJ. Calcium supplements: benefits and risks. J Intern Med. 2015; 278:354–368.
Article23. Lorente-Poch L, Sancho JJ, Ruiz S, Sitges-Serra A. Importance of in situ preservation of parathyroid glands during total thyroidectomy. Br J Surg. 2015; 102:359–367.
Article24. Gu J, Wang J, Nie X, Wang W, Shang J. Potential role for carbon nanoparticles identification and preservation in situ of parathyroid glands during total thyroidectomy and central compartment node dissection. Int J Clin Exp Med. 2015; 8:9640–9648.25. Kuriloff DB, Sanborn KV. Rapid intraoperative localization of parathyroid glands utilizing methylene blue infusion. Otolaryngol Head Neck Surg. 2004; 131:616–622.
Article26. Grubbs EG, Mittendorf EA, Perrier ND, Lee JE. Gamma probe identification of normal parathyroid glands during central neck surgery can facilitate parathyroid preservation. Am J Surg. 2008; 196:931–935.
Article27. Ladurner R, Hallfeldt KK, Al Arabi N, Stepp H, Mueller S, Gallwas JK. Optical coherence tomography as a method to identify parathyroid glands. Lasers Surg Med. 2013; 45:654–659.
Article28. Grodski S, Farrell S. Early postoperative PTH levels as a predictor of hypocalcaemia and facilitating safe early discharge after total thyroidectomy. Asian J Surg. 2007; 30:178–182.
Article29. Wang TS, Cayo AK, Wilson SD, Yen TW. The value of postoperative parathyroid hormone levels in predicting the need for long-term vitamin D supplementation after total thyroidectomy. Ann Surg Oncol. 2011; 18:777–781.
Article30. Roh JL, Park CI. Intraoperative parathyroid hormone assay for management of patients undergoing total thyroidectomy. Head Neck. 2006; 28:990–997.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postoperative Hypoparathyroidism and the Viability of the Parathyroid Glands During Thyroidectomy
- Hypoparathyroidism after Thyroidectomy and the Effect of Parathyroid Autotransplantation
- Characteristics of Hypoparathyroidism after Total Thyroidectomy with or without Hashimoto Thyroiditis
- Transient Hypocalcemia after Thyroidectomy
- Percentage Decline of Parathyroid Hormone Level is a Predictor for Post-thyroidectomy Symptomatic Hypocalcemia
