The Central Dislocation of Femoral Head in the Transverse and Both Column Acetabular Fractures: Is It Really Medialized?
- Affiliations
-
- 1Department of Orthopaedics and Traumatology, Kocaeli University School of Medicine, Izmit, Kocaeli, Turkey. drozgurselek@gmail.com
- 2Department of Orthopaedics and Traumatology, Akademi Hospital, Izmit, Kocaeli, Turkey.
- KMID: 2389524
- DOI: http://doi.org/10.5371/hp.2017.29.3.182
Abstract
- PURPOSE
We hypothesized that the central dislocation of the femoral head does generally not occur in transverse acetabular fractures, although it does usually occur in both column fractures.
MATERIALS AND METHODS
Fifty-two transverse and both column acetabular fracture cases were evaluated retrospectively. The distances between (a) the sciatic notch on the fracture side and the vertical axis of the pelvis (VA line) and (b) the contralateral intact sciatic notch and the VA line were measured. The a/b ratio corresponded to the superior iliac segment displacement or rotation. The ratio of the distance between the fracture side femoral head and the VA line (c) and the distance between the contralateral intact femoral head and the VA line (d) corresponded to the femoral head displacement. The width of ischium (e) on fractured side and (f) contralateral side were measured. The e/f ratio increment reflected ischiadic fragment mobility.
RESULTS
The median value of femoral head displacement (c/d) of the transverse fracture group (n=25) was 1.02 (1.000-1.07). Ischiadic fragment rotation (e/f ratio) of the transverse fracture group was 1.000. The median value of femoral head displacement (c/d) of the both column fractures (n=27) was 0.78 (0.64-0.85). Ischiadic fragment rotation (e/f ratio) of the both-column group was 1.15 (1.06-1.23). The differences between groups according to measurements were statistically significant.
CONCLUSION
In contrary to Letournel description, our findings showed no medialization of femoral head in transverse acetabular fractures in general. This might be an illusion resulting from external rotation of the superior iliac segment.
Keyword
Figure
-
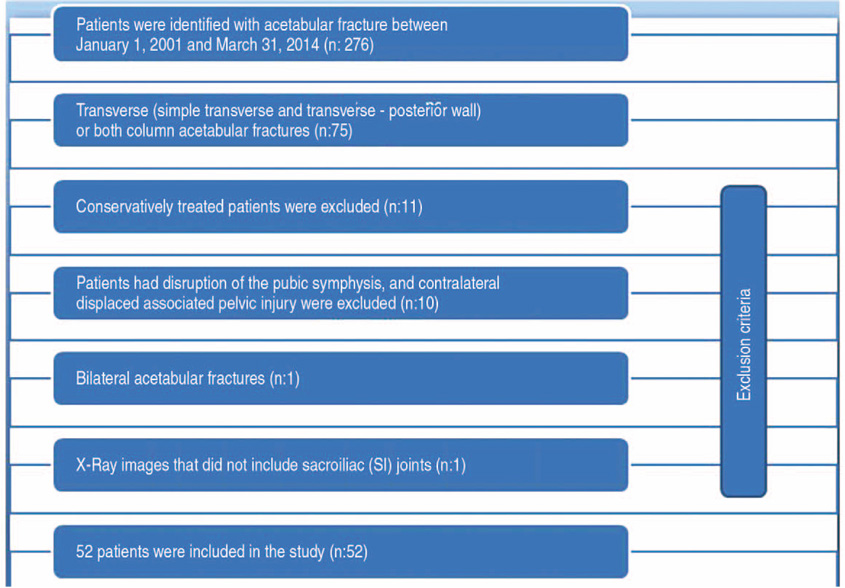
Fig. 1 Flow diagram of the exclusion criteria.
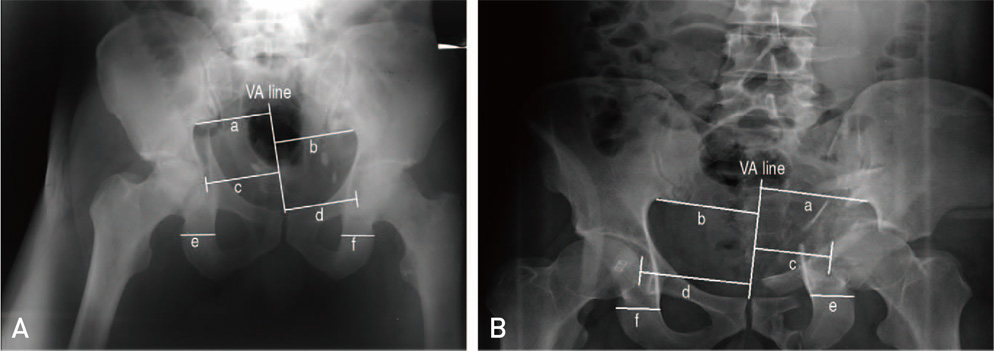
Fig. 2 The method of the measurements from anteroposterior (AP) radiography. The distance between the fractured side sciatic notch and the vertical axis of the pelvis (VA line) was named as “a” and the distance between the VA line and the contralateral intact sciatic notch was named as “b”. The distance between the medial border of the fractured side femoral head and VA line was named as “c” and the distance between the VA line and the medial border of the contralateral intact femoral head was named as “d”. The width of ischium “e” on fractured side and contralateral side “f”. (A) Preoperative AP radiography of transverse type acetabular fracture; a/b ratio: 0.97, c/d ratio: 1, and e/f ratio: 1. (B) Preoperative AP radiography of both column type acetabular fracture; a/b ratio: 1.03, c/d ratio: 0.69, and e/f ratio: 1.07.
Reference
-
1. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78:1632–1645.2. Mears DC, Velyvis JH, Chang CP. Displaced acetabular fractures managed operatively: indicators of outcome. Clin Orthop Relat Res. 2003; (407):173–186.
Article3. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am. 1964; 46:1615–1646.4. Bastian JD, Giannoudis PV. Central acetabular fracture dislocations: are existing classifications comprehensive? Injury. 2014; 45:1807–1815.
Article5. Shi HF, Xiong J, Chen YX, Wang JF, Wang YH. Radiographic analysis of the restoration of hip joint center following open reduction and internal fixation of acetabular fractures: a retrospective cohort study. BMC Musculoskelet Disord. 2014; 15:277.
Article6. Dickson KF, Matta JM. Skeletal deformity after anterior external fixation of the pelvis. J Orthop Trauma. 2009; 23:327–332.
Article7. Matta JM, Mehne DK, Roffi R. Fractures of the acetabulum. Early results of a prospective study. Clin Orthop Relat Res. 1986; (205):241–250.8. Pierannunzii L, Fischer F, Tagliabue L, Calori GM, d'Imporzano M. Acetabular both-column fractures: essentials of operative management. Injury. 2010; 41:1145–1149.
Article9. Osgood GM, Manson TT, O'Toole RV, Turen CH. Combined pelvic ring disruption and acetabular fracture: associated injury patterns in 40 patients. J Orthop Trauma. 2013; 27:243–247.10. Suzuki T, Smith WR, Hak DJ, et al. Combined injuries of the pelvis and acetabulum: nature of a devastating dyad. J Orthop Trauma. 2010; 24:303–308.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Acetabular Coverage of the Femoral Head in Sport-Related Posterior Hip Dislocation or Subluxation
- Single Percutaneous Retrograde Anterior Column Screw Fixation in a Minimally Displaced Transverse Acetabular Fracture - A Case Report -
- Combined Femoral and Sciatic Nerve Palsy Associated with Acetabular Fracture and Dislocation: A Case Report
- Osteonecrosis of the Femoral Head in the Setting of a Complex Acetabulum Fracture without Hip Dislocation Treated Surgically Using Ilio-inguinal Approach: A Case Report
- Anatomical Results According to Fracture Pattern after Surgical Treatment of Acetabular Fractures
