Hip Pelvis.
2014 Sep;26(3):185-188. 10.5371/hp.2014.26.3.185.
Osteonecrosis of the Femoral Head in the Setting of a Complex Acetabulum Fracture without Hip Dislocation Treated Surgically Using Ilio-inguinal Approach: A Case Report
- Affiliations
-
- 1Department of Orthopedic Surgery, Konkuk University School of Medicine, Seoul, Korea. damioh@gmail.com
- KMID: 2054183
- DOI: http://doi.org/10.5371/hp.2014.26.3.185
Abstract
- Osteonecrosis in isolated fractures of the acetabulum without dislocation of hip seems to be a known complication, but to our knowledge it has not been reported adequately. The causative nature of post-traumatic femoral head osteonecrosis has not been studied critically. The pathophysiology of osteonecrosis in this case also eludes us. Striking evidence points towards the intra-operative blood loss and low mean arterial pressure possibly leading to hypo-perfusion of femoral head leading to osteonecrosis. Fractures of the acetabulum pose a difficult problem for the patient and the surgeon because of possible complications. Thus any surgeon involved in surgery for fractures of the acetabulum should be aware of the possibility of this potential complication. Here is a 61-year male, who sustained a complex fracture of the acetabulum without hip dislocation, subsequently was treated surgically with internal fixation using an anterior approach, 10 months after surgery patient developed osteonecrosis of the femoral head.
MeSH Terms
Figure
-
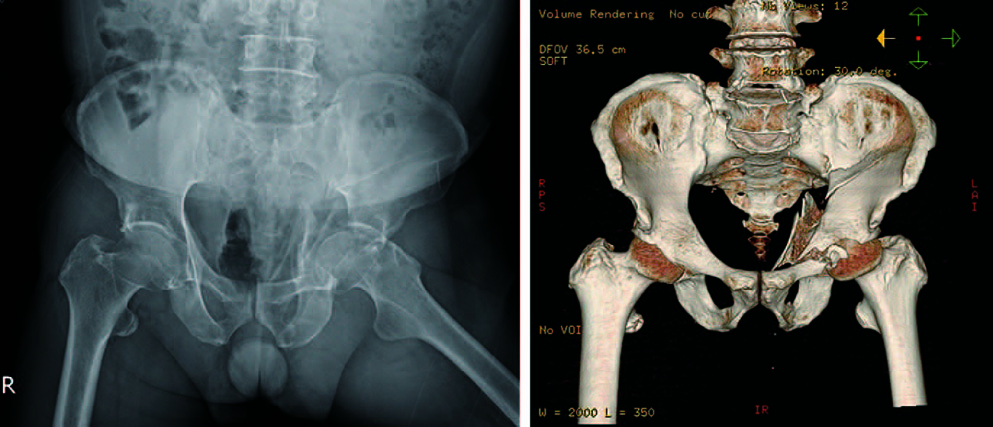
Fig. 1 Preoperative images. (A) X-ray image. (B) Computed tomography scan.
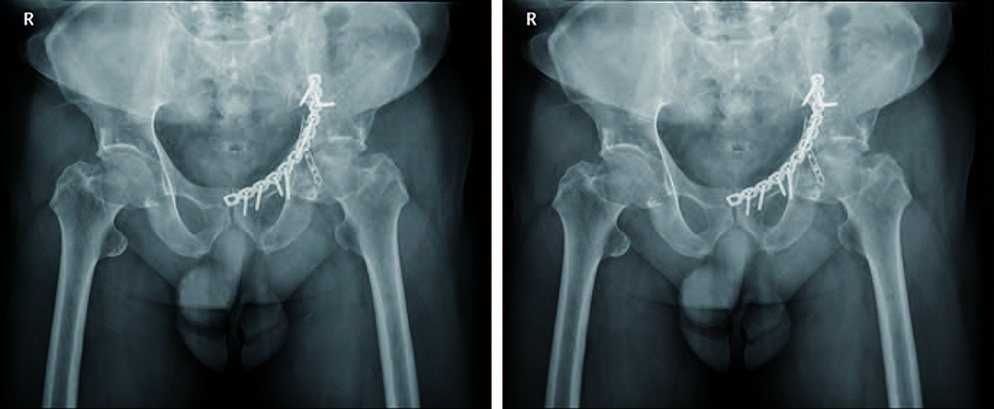
Fig. 2 Postoperative images. (A) X-ray image of immediately after surgery. (B) X-ray image after 10 months.
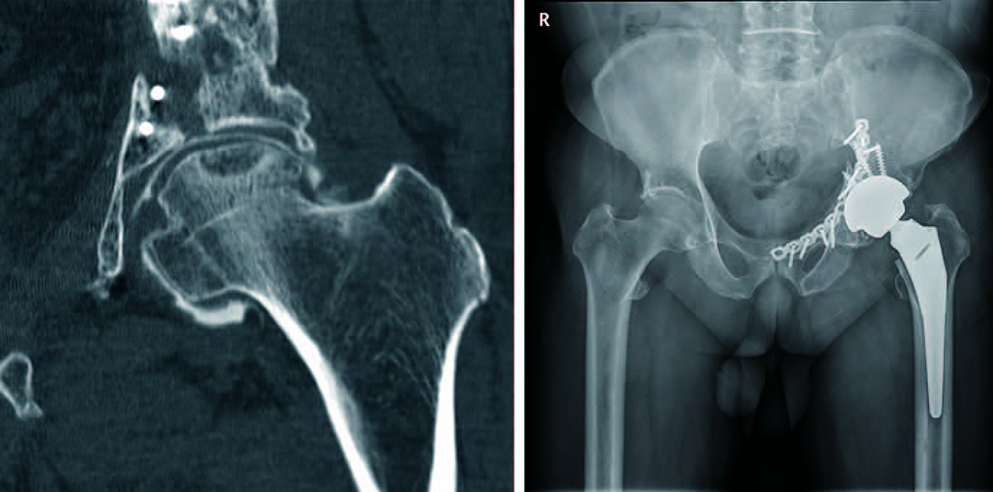
Fig. 3 (A) Computed tomography scan showing osteonecrosis of the femoral head. (B) Postoperative x-ray image after total hip replacement.
Reference
-
1. Judet R, Judet J, Letournel E. Fractures of the acetabulum: classification and surgical approaches for open reduction. Preliminary report. J Bone Joint Surg Am. 1964; 46:1615–1646.2. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical results in patients managed operatively within three weeks after the injury. J Bone Joint Surg Am. 1996; 78:1632–1645.3. Giannoudis PV, Grotz MR, Papakostidis C, Dinopoulos H. Operative treatment of displaced fractures of the acetabulum. A meta-analysis. J Bone Joint Surg Br. 2005; 87:2–9.4. Matta JM, Anderson LM, Epstein HC, Hendricks P. Fractures of the acetabulum. A retrospective analysis. Clin Orthop Relat Res. 1986; 205:230–240.5. Liebergall M, Mosheiff R, Low J, Goldvirt M, Matan Y, Segal D. Acetabular fractures. Clinical outcome of surgical treatment. Clin Orthop Relat Res. 1999; 366:205–216.6. Letournel E, Judet R, Elson R. Fractures of the acetabulum. Berlin, Germany: Springer-Verlag;1981.7. Baumgaertner MR. Fractures of the posterior wall of the acetabulum. J Am Acad Orthop Surg. 1999; 7:54–65.
Article8. Trueta J, Harrison MH. The normal vascular anatomy of the femoral head in adult man. J Bone Joint Surg Br. 1953; 35-B:442–461.
Article9. Kenzora JE, Glimcher MJ. Accumulative cell stress: the multifactorial etiology of idiopathic osteonecrosis. Orthop Clin North Am. 1985; 16:669–679.
Article10. Orpen N, Walker G, Fairlie N, Coghill S, Birch N. Avascular necrosis of the femoral head after surgery for lumbar spinal stenosis. Spine (Phila Pa 1976). 2003; 28:E364–E367.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior Hip Dislocation with Ipsilateral Fractures of the Femoral Head and Intertrochanter: A Case Report
- Posttraumatic Osteonecrosis of the Femoral Head after Nine Years of Posterior Femoral Head Fracture Dislocation
- Surgical Treatment of the Posterior wall Fracture of Acetabulum with Posterior Hip Dislocation
- Osteonecrosis of Femoral Head after Pelvic Fracture: A Case Report
- A Traumatic Anterior Hip Dislocation Associated Ipsilateral Femoral Shaft Segmental Fracture : Case Report
