Endoscopic Management of Gastrointestinal Leaks and Perforation with Polyglycolic Acid Sheets
- Affiliations
-
- 1Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea. hschungmd@gmail.com
- 2Institute of Gastroenterology, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2388827
- DOI: http://doi.org/10.5946/ce.2016.121
Abstract
- Gastrointestinal (GI) leakage, fistulae, and perforations can be serious and life threatening. There has been a paradigm shift in the management approach of these conditions, from surgical to conservative, including endoscopic management. Here, we report two cases of endoscopic closure of a GI fistula and perforation using polyglycolic acid (PGA) sheets with fibrin glue. The first case is of an anastomotic leak detected after subtotal gastrectomy with gastroduodenostomy. After failed application of endoclips, a PGA sheet was applied, and the fistula was successfully closed. The second case was of a 15-mm large perforated gastric ulcer, which was also successfully closed with a PGA sheet. This is the first case report that PGA sheet was used for the treatment of overt perforation. The outcome of these cases suggest that endoscopic closure using PGA sheets can be considered as a useful alternative for the management of GI leakage, fistulae, and perforations.
Keyword
MeSH Terms
Figure
-
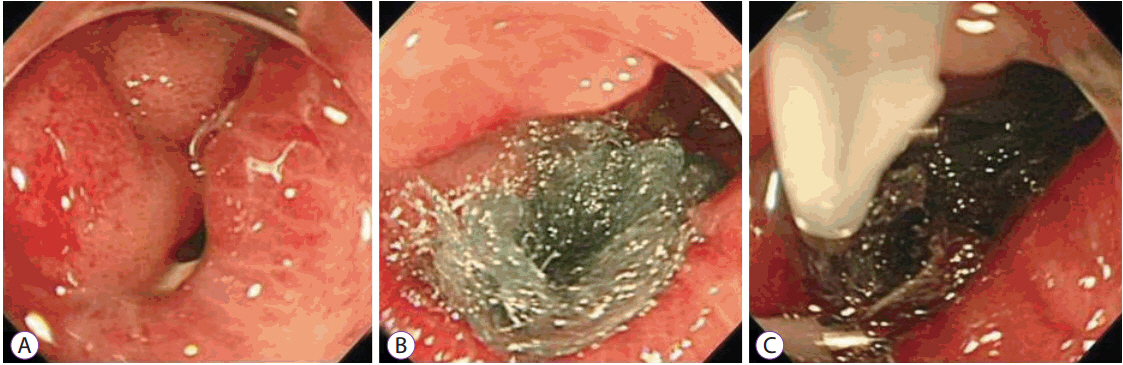
Fig. 1. Endoscopic views after endoscopic closure of the fistula. (A) A fistula after endoscopic closure using endoclips and fibrin glue. Endoclips and fibrin glue applied in the previous endoscopy have disappeared. (B) The polyglycolic acid (PGA) sheet placed to cover the fistula and (C) The fistula covered by the PGA sheet and fibrin glue.

Fig. 2. Fluoroscopic views showing. (A) leakage before closure of the fistula. (B) No leakage of dye after closure of the fistula using polyglycolic acid (PGA) sheet.

Fig. 3. Endoscopic view of closure of the fistula 2 months after endoscopic closure.

Fig. 4. (A) Abdominal–pelvic computed tomography (CT) showing gastric perforation. (B) Endoscopic view showing the 15-mm perforated ulcer at the lesser curvature. (C) Polyglycolic acid (PGA) sheet delivered to the perforation site using an overtube. (D) PGA sheet applied on the perforation site; (E) Endoclips applied at the edge of the PGA sheet for strong adherence, and fibrin glue applied.

Fig. 5. Endoscopic view showing successful closure of the perforation.
Reference
-
1. Hayashibe A, Kameyama M, Shinbo M, Makimoto S. The clinical research for prevention of bile leakage occurred from cut surface of remnant liver (the usefulness of fibrin glue and polyglycolic acid felt as topical sealant). Surgery. 2006; 68:1325–1329.2. Itano H. The optimal combined application technique of fibrin glue and bioabsorbable felt against alveolar air leakage. Eur J Cardiothorac Surg. 2008; 33:457–460.
Article3. Tokushima T. Clinical examination of combined approach using Bolheal and Neoveil on closure of pulmonary fistula in chest surgery. Ther Res. 2004; 25:2245–2249.4. Takeuchi J, Suzuki H, Murata M, et al. Clinical evaluation of application of polyglycolic acid sheet and fibrin glue spray for partial glossectomy. J Oral Maxillofac Surg. 2013; 71:e126–e131.
Article5. Takimoto K, Toyonaga T, Matsuyama K. Endoscopic tissue shielding to prevent delayed perforation associated with endoscopic submucosal dissection for duodenal neoplasms. Endoscopy. 2012; 44 Suppl 2 UCTN:E414–E415.
Article6. Tsuji Y, Ohata K, Gunji T, et al. Endoscopic tissue shielding method with polyglycolic acid sheets and fibrin glue to cover wounds after colorectal endoscopic submucosal dissection (with video). Gastrointest Endosc. 2014; 79:151–155.
Article7. Iizuka T, Kikuchi D, Yamada A, Hoteya S, Kajiyama Y, Kaise M. Polyglycolic acid sheet application to prevent esophageal stricture after endoscopic submucosal dissection for esophageal squamous cell carcinoma. Endoscopy. 2015; 47:341–344.
Article8. Fukumoto R, Orlina J, McGinty J, Teixeira J. Use of polyflex stents in treatment of acute esophageal and gastric leaks after bariatric surgery. Surg Obes Relat Dis. 2007; 3:68–71. discussion 71-72.
Article9. Arezzo A, Verra M, Reddavid R, Cravero F, Bonino MA, Morino M. Efficacy of the over-the-scope clip (OTSC) for treatment of colorectal postsurgical leaks and fistulas. Surg Endosc. 2012; 26:3330–3333.
Article10. Fernandez-Esparrach G, Lautz DB, Thompson CC. Endoscopic repair of gastrogastric fistula after Roux-en-Y gastric bypass: a less-invasive approach. Surg Obes Relat Dis. 2010; 6:282–288.
Article11. Eleftheriadis E, Tzartinoglou E, Kotzampassi K, Aletras H. Early endoscopic fibrin sealing of high-output postoperative enterocutaneous fistulas. Acta Chir Scand. 1990; 156:625–628.12. Tsujii Y, Kato M, Shinzaki S, et al. Polyglycolic acid sheets for repair of refractory esophageal fistula. Endoscopy. 2015; 47 Suppl 1 UCTN:E39–E40.
Article13. Nakagawa Y, Nagai T, Soma W, et al. Endoscopic closure of a large ERCP-related lateral duodenal perforation by using endoloops and endoclips. Gastrointest Endosc. 2010; 72:216–217.
Article14. Yonezawa H, Yanamoto S, Kawasaki G, Umeda M. Polyglycolic acid sheets with fibrin glue (MCFP technique) for resection of oral mucosa. Br J Oral Maxillofac Surg. 2012; 50:e43–e44.
Article15. Kocer B, Surmeli S, Solak C, et al. Factors affecting mortality and morbidity in patients with peptic ulcer perforation. J Gastroenterol Hepatol. 2007; 22:565–570.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The use of OverStitchâ„¢ for the treatment of intestinal perforation, fistulas and leaks
- Efficacy of the Envelope Method in Applying Polyglycolic Acid Sheets to Post-Endoscopic Submucosal Dissection Ulcers in Living Pigs
- Complications of endoscopic resection in the upper gastrointestinal tract
- Endoscopic management of postsurgical leaks
- Management of gastrointestinal tract perforations
