Investig Clin Urol.
2017 Sep;58(5):331-338. 10.4111/icu.2017.58.5.331.
Patient-reported quality of life recovery curves after robotic prostatectomy are similar across body mass index categories
- Affiliations
-
- 1Department of Urology, Geisinger Health System, Danville, PA, USA. tgarg@geisinger.edu
- 2Department of Epidemiology & Health Services Research, Geisinger Health System, Danville, PA, USA.
- 3Biostatistics Core, Biomedical & Translational Informatics Institute, Geisinger Health System, Danville, PA, USA.
- 4Phenomic Analytics & Clinical Data Core, Biomedical & Translational Informatics Institute, Geisinger Health System, Danville, PA, USA.
- 5Biomedical & Translational Informatics Institute, Geisinger Health System, Danville, PA, USA.
- KMID: 2388049
- DOI: http://doi.org/10.4111/icu.2017.58.5.331
Abstract
- PURPOSE
To assess the impact of body mass index (BMI) on postoperative recovery curve of urinary and sexual function after robotic-assisted laparoscopic prostatectomy (RALP). We hypothesized that overweight and obese men have different recovery curves than normal weight men.
MATERIALS AND METHODS
We reviewed preoperative and postoperative surveys from 691 men who underwent RALP from 2004-2014 in an integrated healthcare delivery system. Survey instruments included: sexual health inventory for men (SHIM), urinary behavior, leakage, and incontinence impact questionnaire (IIQ). A repeated measures analysis with autoregressive covariance structure was employed with linear splines with 2 knots for the time factor. We fit unadjusted and adjusted models and stratified by BMI (under/normal weight, overweight, and obese). Adjusted models included age, race/ethnicity, smoking status, diabetes, operation length, prostate-specific antigen, pathologic stage, nerve-sparing status, and surgery year.
RESULTS
Mean age was 59 years. Most men were overweight (43%) and obese (42%). There were no significant differences in mean baseline SHIM, urinary behavior, leakage, and IIQ scores by BMI category. All groups had initial steep declines in urinary and sexual function in the first 3 months after RALP. There were no significant differences in postoperative urinary and sexual function score curves by BMI category.
CONCLUSIONS
The pattern of urinary and sexual function recovery was similar across all BMI categories. Overweight and obese men may be counseled that urinary and sexual function recovery curves after surgery is similar to that of normal weight men.
MeSH Terms
Figure
-
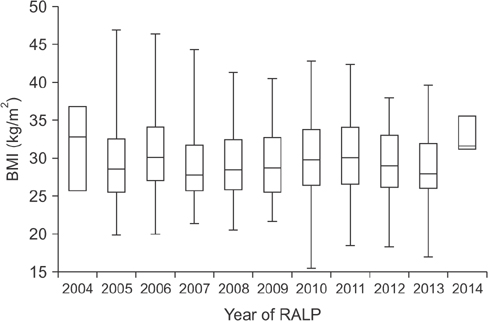
Fig. 1 Median body mass index (BMI) by year of robotic assisted laparoscopic prostatectomy (RALP).
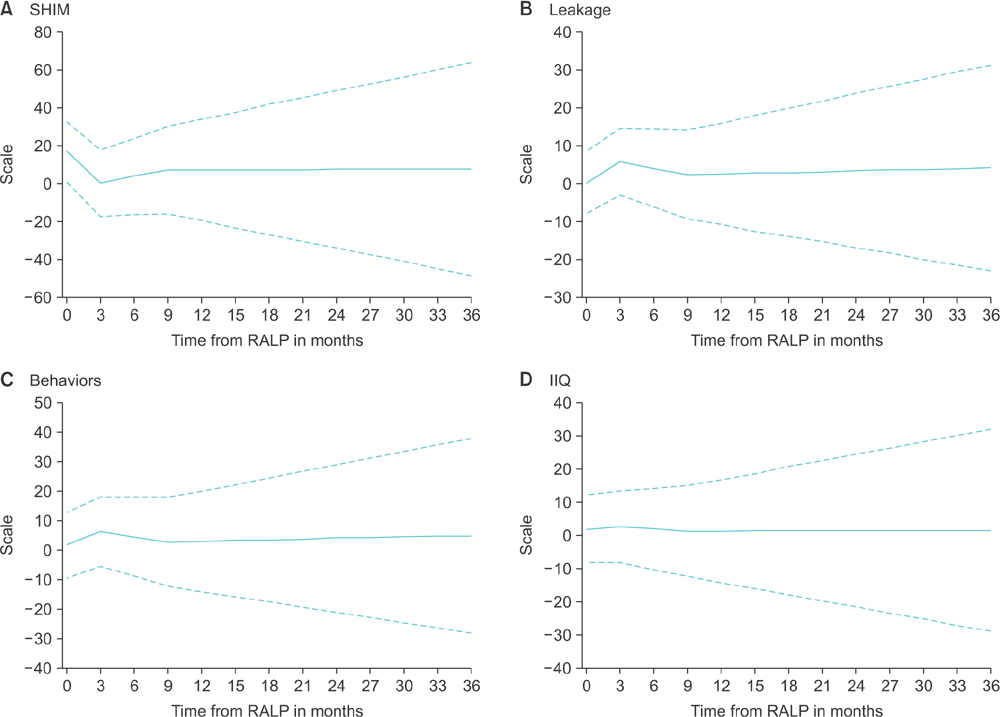
Fig. 2 (A–D) Urinary and sexual function recovery curve after robotic-assisted laparoscopic prostatectomy (RALP) for an averaged patient in the cohort with 95% confidence intervals. SHIM, sexual health inventory for men; IIQ, incontinence impact questionnaire.
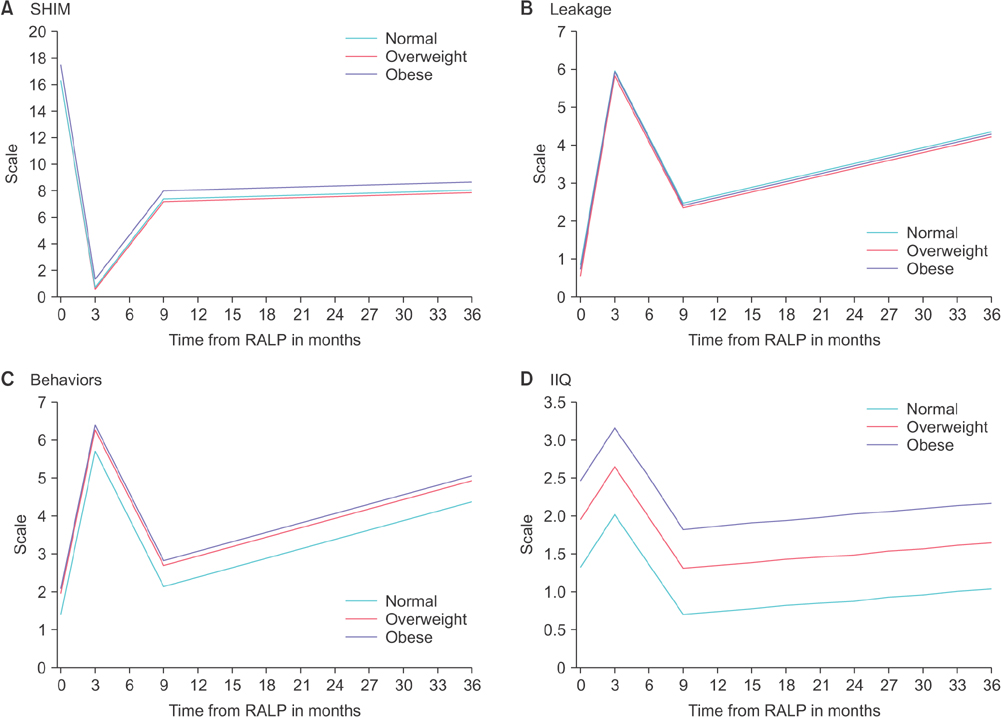
Fig. 3 (A–D) Urinary and sexual function recovery curves after robotic-assisted laparoscopic prostatectomy (RALP) stratified by body mass index (BMI) categories. SHIM, sexual health inventory for men; IIQ, incontinence impact questionnaire. BMI (kg/m2): normal, 18.5–24.9; overweight, 25–29.9; obese, >30.
Reference
-
1. Overweight & obesity: adult obesity facts [Internet]. Atlanta (GA): Centers for Disease Control and Prevention;2017. updated 2016 Sept 1. cited 2016 June 20. Available from: http://www.cdc.gov/obesity/data/adult.html.2. Hamlin RJ, Sprung J, Hofer RE, Schroeder DR, Weingarten TN. Obesity trends in the surgical population at a large academic center : a comparison between 1989-1991 to 2006-2008 epochs. Acta Chir Belg. 2013; 113:397–400.3. Mullen JT, Moorman DW, Davenport DL. The obesity paradox: body mass index and outcomes in patients undergoing nonbariatric general surgery. Ann Surg. 2009; 250:166–172.4. National Comprehensive Cancer Network clinical practice guidelines in oncology (NCCN Guidelines): Prostate cancer (version 1.2016) [Internet]. Fort Wathington (PA): National Comprehensive Cancer Network;c2017. cited 2016 June 20. Available from: http://www.nccn.org/professionals/physician_gls/pdf/prostate.pdf.5. Wiltz AL, Shikanov S, Eggener SE, Katz MH, Thong AE, Steinberg GD, et al. Robotic radical prostatectomy in overweight and obese patients: oncological and validated-functional outcomes. Urology. 2009; 73:316–322.6. Kwon YS, Leapman M, McBride RB, Hobbs AR, Collingwood SA, Stensland KD, et al. Robotic-assisted laparoscopic prostatectomy in men with metabolic syndrome. Urol Oncol. 2014; 32:40.7. Uffort EE, Jensen JC. Impact of obesity on early erectile function recovery after robotic radical prostatectomy. JSLS. 2011; 15:32–37.8. Barry MJ, Fowler FJ Jr, O'Leary MP, Bruskewitz RC, Holtgrewe HL, Mebust WK, et al. The American Urological Association symptom index for benign prostatic hyperplasia. The Measurement Committee of the American Urological Association. J Urol. 1992; 148:1549–1557.9. Rosen RC, Cappelleri JC, Smith MD, Lipsky J, Peña BM. Development and evaluation of an abridged, 5-item version of the International Index of Erectile Function (IIEF-5) as a diagnostic tool for erectile dysfunction. Int J Impot Res. 1999; 11:319–326.10. Moore KN, Jensen L. Testing of the Incontinence Impact Questionnaire (IIQ-7) with men after radical prostatectomy. J Wound Ostomy Continence Nurs. 2000; 27:304–312.11. Stewart WF, Van Rooyen JB, Cundiff GW, Abrams P, Herzog AR, Corey R, et al. Prevalence and burden of overactive bladder in the United States. World J Urol. 2003; 20:327–336.12. Lee JK, Assel M, Thong AE, Sjoberg DD, Mulhall JP, Sandhu J, et al. Unexpected long-term improvements in urinary and erectile function in a large cohort of men with self-reported outcomes following radical prostatectomy. Eur Urol. 2015; 68:899–905.13. Moskovic DJ, Lavery HJ, Rehman J, Nabizada-Pace F, Brajtbord J, Samadi DB. High body mass index does not affect outcomes following robotic assisted laparoscopic prostatectomy. Can J Urol. 2010; 17:5291–5298.14. Mikhail AA, Stockton BR, Orvieto MA, Chien GW, Gong EM, Zorn KC, et al. Robotic-assisted laparoscopic prostatectomy in overweight and obese patients. Urology. 2006; 67:774–779.15. Sundi D, Reese AC, Mettee LZ, Trock BJ, Pavlovich CP. Laparoscopic and robotic radical prostatectomy outcomes in obese and extremely obese men. Urology. 2013; 82:600–605.16. Boorjian SA, Crispen PL, Carlson RE, Rangel LJ, Karnes RJ, Frank I, et al. Impact of obesity on clinicopathologic outcomes after robot-assisted laparoscopic prostatectomy. J Endourol. 2008; 22:1471–1476.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Functional recovery after radical prostatectomy for prostate cancer
- Changes in health-related quality of life after radical prostatectomy for prostate cancer: A longitudinal cohort study in Korea
- Initial experience with Retzius-sparing robot-assisted radical prostatectomy compared to the conventional method: is it a suitable option for robotic prostatectomy beginners?
- Effect of Posterior Urethral Reconstruction (PUR) in Early Recovery of Urinary Continence after Robotic-Assisted Radical Prostatectomy
- Robotic Prostatectomy in a Patient with a Miles' Operation
