Ann Surg Treat Res.
2017 Aug;93(2):98-102. 10.4174/astr.2017.93.2.98.
Early experience of transilluminated cryosurgery for varicose vein with saphenofemoral reflux: review of 84 patients (131 limbs)
- Affiliations
-
- 1Department of Surgery, Hallym University Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. Kimjiw96@hallym.or.kr
- KMID: 2387340
- DOI: http://doi.org/10.4174/astr.2017.93.2.98
Abstract
- PURPOSE
Varicose veins with great saphenous vein (GSV) insufficiency is prevalent. Among various surgical treatments for varicose veins, cryosurgery of GSV is an alternative minimally invasive technique that could leave fewer scars and replace conventional stripping with ambulatory phlebectomy. This study sought to assess outcomes including efficacy and safety of cryosurgery for varicose veins.
METHODS
One hundred thirty-one limbs in 84 patients (37 male, 47 female; mean age, 53.3 years) with varicose veins were treated with cryosurgery over a 2-year period. The patients were followed for postoperative complication with surveillance of recurrence. The analyzed variables included age, sex, symptom, operative time (from skin incision to the application of elastic bandages on the legs for compression purposes), and postoperative complications including bruising, hematoma, superficial thrombophlebitis, cellulitis, seroma, cutaneous nerve damage, and wound complication.
RESULTS
The mean operative time was 64.7 minutes for both limbs and 44 minutes for single limbs. The median number of incisions was 2. For stripping of GSV, one incision at the groin was necessary. Postoperative complications included an episode of hematoma in 3 limbs (2.3%), cutaneous nerve damage in 3 limbs (2.3%), cellulitis in 2 patients (1.5%), and seroma in 1 limb (0.8%). No wound infection, thrombophlebitis or deep venous thrombosis was observed. During follow-up (mean follow-up period, 13.5 months; range, 3-28 months), there was no recurrence.
CONCLUSION
Cryosurgery to treat varicose veins is an effective and safe treatment modality in terms of postoperative complication, cosmetic result, and recurrence.
MeSH Terms
Figure
-

Fig. 1 The cryomachine and cryoprobe used for the cryosurgery of varicose vein (MetrumCryoFlex; Spolka, Blizne, Poland).
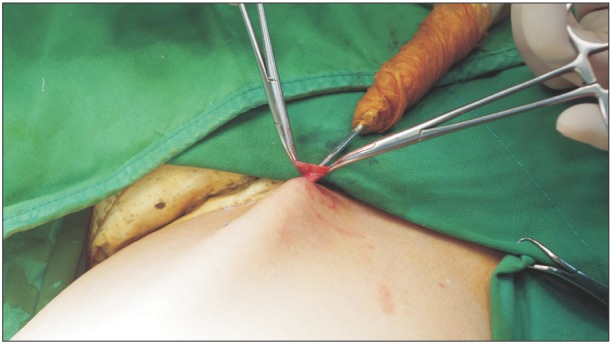
Fig. 2 A long cryoprobe is inserted into the lumen of greater saphenous vein with care to avoid vein perforation after all the collaterals are separated, ligated and cut off to prevent recurrence.

Fig. 3 Picture of removed greater saphenous vein. After freezing, the cryoprobe is pulled out by a sharp jerky movement.

Fig. 4 The superficial varicosities is pulled out by slightly rotating the probe after freezing. Irrigationillumination device allows the operator to visualize the vein and accurate placement of additional stab incisions.

Fig. 5 Picture of removed superficial varicosities.
Reference
-
1. Disselhoff BC, der Kinderen DJ, Kelder JC, Moll FL. Randomized clinical trial comparing endovenous laser with cryostripping for great saphenous varicose veins. Br J Surg. 2008; 95:1232–1238. PMID: 18763255.
Article2. Park HS, Kwon Y, Eom BW, Lee T. Prosepctive nonrandomized comparison of quality of life and recurrence between high ligation and stripping and radiofrequency ablation for varicose veins. J Korean Surg Soc. 2013; 84:48–56. PMID: 23323236.3. Beale RJ, Gough MJ. Treatment options for primary varicose veins-a review. Eur J Vasc Endovasc Surg. 2005; 30:83–95. PMID: 15933989.
Article4. Schouten R, Mollen RM, Kuijpers HC. A comparison between cryosurgery and conventional stripping in varicose vein surgery: perioperative features and complications. Ann Vasc Surg. 2006; 20:306–311. PMID: 16779510.
Article5. Etienne G, Constantin JM, Hevia M. Cryostripping: an advance in the treatment of varicose veins. 3811 operated limbs. Presse Med. 1995; 24:1017–1020. PMID: 7667227.6. Robertson LA, Evans CJ, Lee AJ, Allan PL, Ruckley CV, Fowkes FG. Incidence and risk factors for venous reflux in the general population: edinburgh vein study. Eur J Vasc Endovasc Surg. 2014; 48:208–214. PMID: 24951373.
Article7. Evans CJ, Fowkes FG, Ruckley CV, Lee AJ. Prevalence of varicose veins and chronic venous insufficiency in men and women in the general population: Edinburgh Vein Study. J Epidemiol Community Health. 1999; 53:149–153. PMID: 10396491.
Article8. Callan MJ. Epidemiology of varicose veins. Br J Surg. 1994; 81:167–173. PMID: 8156326.9. Yi EJ, Lee SH, Cho JH, Kim KT. Early results of cryosurgery in varicose veins in Korea: safety and feasibility. Korean J Thorac Cardiovasc Surg. 2012; 45:155–160. PMID: 22708082.
Article10. Garde C. Cryosurgery of varicose veins. J Dermatol Surg Oncol. 1994; 20:56–58. PMID: 8288809.
Article11. Merchant RF, Depalma RG, Kabnick LS. Endovascular obliteration of saphenous reflux: a multicenter study. J Vasc Surg. 2002; 35:958–965. PMID: 12021712.
Article12. Min RJ, Zimmet SE, Isaacs MN, Forrestal MD. Endovenous laser treatment of the incompetent great saphenous vein. J Vasc Interv Radiol. 2001; 12:1167–1171. PMID: 11585882.13. Rautio T, Ohinmaa A, Perala J, Ohtonen P, Heikkinen T, Wiik H, et al. Endovenous obliteration versus conventional stripping operation in treatment of primary varicose veins: a randomized controlled trial with comparison of the costs. J Vasc Surg. 2002; 35:958–965. PMID: 12021712.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Recent Overview of Varicose Vein in the Legs
- The Evaluation of the Saphenofemoral Junction after Endovenous Laser Treatment for Varicose Veins and Its Clinical Significance
- The Pattern & Change of Venous Reflux in Primary Varicose Vein
- Clinical Experiences of Transilluminated Powered Phlebectomy in Varicose Vein
- Early Results of Cryosurgery in Varicose Veins in Korea: Safety and Feasibility
