Phenylephrine Induced Posterior Reversible Encephalopathy Syndrome during Resection of Solitary Pulmonary Nodule
- Affiliations
-
- 1Department of Neurology, Konyang University College of Medicine, Daejeon, Korea. nukedoc@hanmail.net
- KMID: 2385884
- DOI: http://doi.org/10.18700/jnc.170005
Abstract
- BACKGROUND
Posterior reversible encephalopathy syndrome (PRES) is a neurological complication caused by cerebral hyperperfusion.
CASE REPORT
A 46-year-old male presented with decreased mental status, left facial palsy, and left-sided weakness after video-assisted thoracoscopic surgery for a solitary pulmonary nodule. During the surgery, phenylephrine was infused intravenously for general anesthesia-induced hypotension. High signal intensity at the right parietooccipital lobe was noted on fluid-attenuated inversion recovering imaging and diffusion-weighted imaging. His neurological symptoms improved two days after initial presentation. Follow-up diffusion-weighted imaging showed resolution of the brain lesions 10 days after the surgery.
CONCLUSIONS
We report a patient who presented with PRES after administration of phenylephrine during resection of a solitary pulmonary nodule. PRES should be considered for patients presented with acute neurologic symptoms following surgical procedures.
MeSH Terms
Figure
-
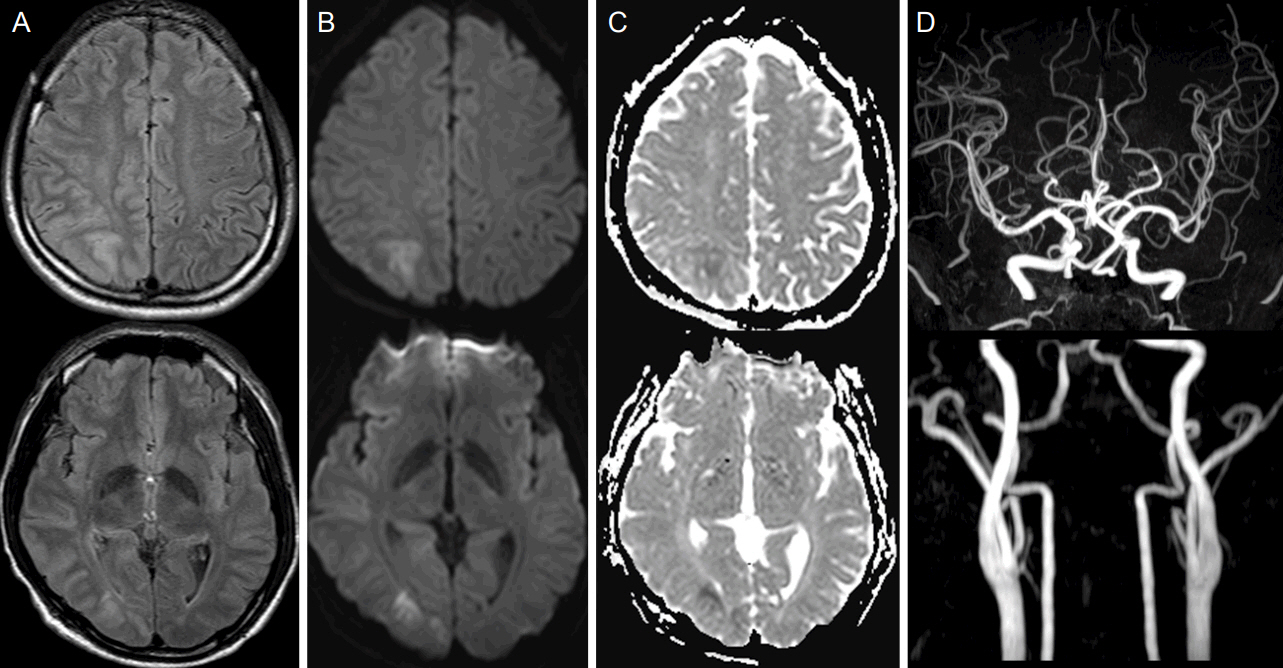
Figure 1. Brain MRI and MRA of the patient at the symptom onset. Fluid-attenuated inversion recovering imaging (FLAIR) (A) and diffusion-weighted imaging (DWI) showed regional hyperintensity in the right parietooccipital area (B), and apparent diffusion coefficent (ADC) map in corresponding area showed hypointense signal, suggesting cytotoxic edema (C). MRA angiography shows normal findings in the intracranial and internal carotid arteries (D). MRI, magnetic resonance imaging; MRA, magnetic resonance angiography.

Figure 2. Follow-up MRI of the patient after 10 days. DWI showed decreased signal intensities in the right parietoocipital subcortical area (A), and the ADC map were almost resolved, except for small foci of cerebral infarction (B). DWI, diffusion-weighted imaging; ADC, apparent diffusion coefficient.
Reference
-
1. Fugate JE, Rabinstein AA. Posterior reversible encephalopathy syndrome: clinical and radiological manifestations, pathophysiology, and outstanding questions. Lancet Neurol. 2015; 14:914–25.
Article2. Fugate JE, Claassen DO, Cloft HJ, Kallmes DF, Kozak OS, Rabinstein AA. Posterior reversible encephalopathy syndrome: associated clinical and radiologic findings. Mayo Clin Proc. 2010; 85:427–32.
Article3. Rabinstein AA, Mandrekar J, Merrell R, Kozak OS, Durosaro O, Fugate JE. Blood pressure fluctuations in posterior reversible encephalopathy syndrome. J Stroke Cerebrovasc Dis. 2012; 21:254–8.
Article4. Gharabawy R, Pothula VR, Rubinshteyn V, Silverberg M, Gave AA. Epinephrine-induced posterior reversible encephalopathy syndrome: a case report. J Clin Anesth. 2011; 23:505–7.
Article5. Triquenot-Bagan A, Gerardin E, Guegan-Massardier E, Onnient Y, Leroy F, Mihout B. Postoperative reversible posterior leukoencephalopathy syndrome. Cerebrovasc Dis. 2003; 16:430–2.
Article6. Kastrup O, Schlamann M, Moenninghoff C, Forsting M, Goericke S. Posterior reversible encephalopathy syndrome: the spectrum of MR imaging patterns. Clin Neuroradiol. 2015; 25:161–71.
Article7. Allman KG, Wilson IH. Oxford Handbook of Anaesthesia. 3rd ed. New York: Oxford university press;2011. p. 367–8.8. Oderich GS, Pereira AA, Rabinstein AA, Mendes BC, Pulido JN. Posterior reversible encephalopathy syndrome from induced hypertension during endovascular thoracoabdominal aortic aneurysm repair. J Vasc Surg. 2015; 61:1062–5.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Posterior reversible encephalopathy syndrome and reversible cerebral vasoconstriction syndrome associated with acute exacerbation of chronic obstructive pulmonary disease
- Posterior Reversible Encephalopathy Syndrome in a Patient with Intoxication of Arisaema amurense
- Hypertension-induced Posterior Reversible Encephalopathy Syndrome
- Posterior Reversible Encephalopathy after Quetiapine Overdose
- Posterior Reversible Encephalopathy Syndrome after Massive Blood Transfusion in a Normotensive Patient
