J Endocr Surg.
2017 Jun;17(2):42-56. 10.16956/jes.2017.17.2.42.
Medico-Legal Issues of Intraoperative Neuromonitoring in Thyroid Surgery
- Affiliations
-
- 1Korea University Medical Center (KUMC) Thyroid Center, Korea University Anam Hospital, Korea University College of Medicine, Seoul, Korea.
- 2Division of Thyroid Surgery, Jilin Provincial Key Laboratory of Surgical Translational Medicine, China-Japan Union Hospital of Jilin University, Changchun, China.
- 3Department of Otolaryngology, Kaohsiung Medical University Hospital, Kaohsiung Medical University, Kaohsiung, Taiwan.
- 4Department of Surgery, Seoul Metropolitan Government-Seoul National University Boramae Medical Center, Seoul, Korea.
- 5Department of Surgery, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Otolaryngology-Head and Neck Surgery, The Johns Hopkins University School of Medicine, Baltimore, MD, USA.
- 7Endocrine Surgery, Universitätsklinikum Essen AöR Medizinisches Zentrum, Essen, Germany.
- 81st Division of General Surgery, Research Center for Endocrine Surgery, Department of Medicine and Surgery, ASST dei Sette Laghi Ospedale di Circolo e Fondazione Macchi, Polo Universitario, University of Insubria (Varese-Como), Varese, Italy. gianlorenzo.dionigi@uninsubria.it
- KMID: 2383821
- DOI: http://doi.org/10.16956/jes.2017.17.2.42
Abstract
- Advances in intraoperative neuromonitoring (IONM) in thyroid surgery have provided significant insights into recurrent laryngeal nerve function during thyroid surgery. Despite the limitations and necessary caution when using intraoperative monitors to interpret neural function, these technologies have been definite steps in the right direction for assessing neural integrity and safe surgical strategy during thyroid operations. The techniques discussed minimize the adverse sequelae of a variety of thyroid gland procedures, reducing the morbidity rates/risks in the perioperative period. Furthermore, it is likely that such monitoring will become a standard of care. Accurate, reliable and continuous monitoring is essential, and on-going large studies with definable end points will be necessary. The use of monitoring, such as continuous one, may improve cost efficiency by reducing permanent nerve injuries. A danger in this process, however, is the potential for public opinion, outside regulatory bodies, or medico-legal implications to drive change and enforce standards of care before appropriate data are available.
Keyword
MeSH Terms
Figure
-
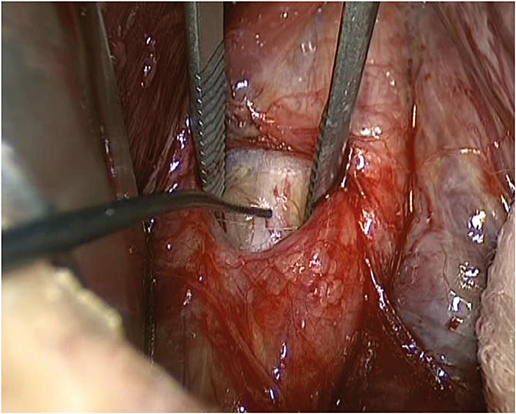
Fig. 1 Pre-dissection VN stimulation (V1). VN = vagal nerve.
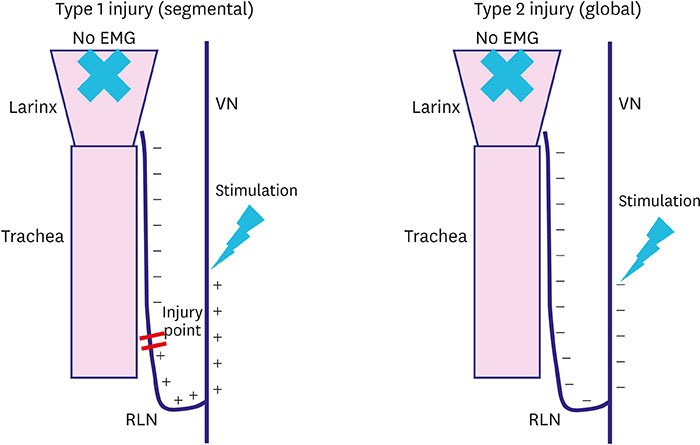
Fig. 2 Type 1 and type 2 injuries. EMG = electromyogram; RLN = recurrent laryngeal nerve; VN = vagal nerve.

Fig. 3 Troubleshooting algorithm in case of loss of EMG signal. EMG = electromyogram; RLN = recurrent laryngeal nerve; LOS = loss of signal; LT = laryngeal twitch.
Cited by 1 articles
-
The Consistency of Intraoperative Neural Monitoring in Thyroid Surgery
Gianlorenzo Dionigi, Young Jun Chai, Francesco Freni, Özer Makay, Bruno Galletti, Francesco Galletti, Hoon Yub Kim
J Endocr Surg. 2018;18(2):91-97. doi: 10.16956/jes.2018.18.2.91.
Reference
-
1. Singer MC, Iverson KC, Terris DJ. Thyroidectomy-related malpractice claims. Otolaryngol Head Neck Surg. 2012; 146:358–361.
Article2. Abadin SS, Kaplan EL, Angelos P. Malpractice litigation after thyroid surgery: the role of recurrent laryngeal nerve injuries, 1989–2009. Surgery. 2010; 148:718–722.
Article3. Randolph GW, Dralle H; International Intraoperative Monitoring Study Group. Electrophysiologic recurrent laryngeal nerve monitoring during thyroid and parathyroid surgery: international standards guideline statement. Laryngoscope. 2011; 121:Suppl 1. S1–S16.
Article4. Tomoda C, Hirokawa Y, Uruno T, Takamura Y, Ito Y, Miya A, et al. Sensitivity and specificity of intraoperative recurrent laryngeal nerve stimulation test for predicting vocal cord palsy after thyroid surgery. World J Surg. 2006; 30:1230–1233.
Article5. Barczyński M, Konturek A, Cichoń S. Randomized clinical trial of visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy. Br J Surg. 2009; 96:240–246.
Article6. Dralle H, Sekulla C, Lorenz K, Brauckhoff M, Machens A; German IONM Study Group. Intraoperative monitoring of the recurrent laryngeal nerve in thyroid surgery. World J Surg. 2008; 32:1358–1366.
Article7. Dralle H, Sekulla C, Lorenz K, Nguyen Thanh P, Schneider R, Machens A. Loss of the nerve monitoring signal during bilateral thyroid surgery. Br J Surg. 2012; 99:1089–1095.
Article8. Godballe C, Madsen AR, Sørensen CH, Schytte S, Trolle W, Helweg-Larsen J, et al. Risk factors for recurrent nerve palsy after thyroid surgery: a national study of patients treated at Danish departments of ENT Head and Neck Surgery. Eur Arch Otorhinolaryngol. 2014; 271:2267–2276.
Article9. Adam MA, Thomas S, Youngwirth L, Hyslop T, Reed SD, Scheri RP, et al. Is there a minimum number of thyroidectomies a surgeon should perform to optimize patient outcomes? Ann Surg. 2017; 265:402–407.
Article10. Lorenz K, Abuazab M, Sekulla C, Schneider R, Nguyen Thanh P, Dralle H. Results of intraoperative neuromonitoring in thyroid surgery and preoperative vocal cord paralysis. World J Surg. 2014; 38:582–591.
Article11. Lorenz K, Sekulla C, Schelle J, Schmeiss B, Brauckhoff M, Dralle H; German Neuromonitoring Study Group. What are normal quantitative parameters of intraoperative neuromonitoring (IONM) in thyroid surgery? Langenbecks Arch Surg. 2010; 395:901–909.
Article12. Brauckhoff M, Machens A, Sekulla C, Lorenz K, Dralle H. Latencies shorter than 3.5 ms after vagus nerve stimulation signify a nonrecurrent inferior laryngeal nerve before dissection. Ann Surg. 2011; 253:1172–1177.
Article13. Chiang FY, Lee KW, Chen HC, Chen HY, Lu IC, Kuo WR, et al. Standardization of intraoperative neuromonitoring of recurrent laryngeal nerve in thyroid operation. World J Surg. 2010; 34:223–229.
Article14. Chiang FY, Lu IC, Kuo WR, Lee KW, Chang NC, Wu CW. The mechanism of recurrent laryngeal nerve injury during thyroid surgery--the application of intraoperative neuromonitoring. Surgery. 2008; 143:743–749.
Article15. Hamelmann WH, Meyer T, Timm S, Timmermann W. A critical estimation of intraoperative neuromonitoring (IONM) in thyroid surgery. Zentralbl Chir. 2002; 127:409–413.
Article16. Thomusch O, Sekulla C, Machens A, Neumann HJ, Timmermann W, Dralle H. Validity of intra-operative neuromonitoring signals in thyroid surgery. Langenbecks Arch Surg. 2004; 389:499–503.
Article17. Beldi G, Kinsbergen T, Schlumpf R. Evaluation of intraoperative recurrent nerve monitoring in thyroid surgery. World J Surg. 2004; 28:589–591.
Article18. Hermann M, Hellebart C, Freissmuth M. Neuromonitoring in thyroid surgery: prospective evaluation of intraoperative electrophysiological responses for the prediction of recurrent laryngeal nerve injury. Ann Surg. 2004; 240:9–17.19. Chan WF, Lang BH, Lo CY. The role of intraoperative neuromonitoring of recurrent laryngeal nerve during thyroidectomy: a comparative study on 1000 nerves at risk. Surgery. 2006; 140:866–872.
Article20. Wong KP, Mak KL, Wong CK, Lang BH. Systematic review and meta-analysis on intra-operative neuro-monitoring in high-risk thyroidectomy. Int J Surg. 2017; 02. 38:21–30.
Article21. Melin M, Schwarz K, Pearson MD, Lammers BJ, Goretzki PE. Postoperative vocal cord dysfunction despite normal intraoperative neuromonitoring: an unexpected complication with the risk of bilateral palsy. World J Surg. 2014; 38:2597–2602.
Article22. Schneider R, Randolph GW, Sekulla C, Phelan E, Thanh PN, Bucher M, et al. Continuous intraoperative vagus nerve stimulation for identification of imminent recurrent laryngeal nerve injury. Head Neck. 2013; 35:1591–1598.
Article23. Dionigi G, Chiang FY, Dralle H, Boni L, Rausei S, Rovera F, et al. Safety of neural monitoring in thyroid surgery. Int J Surg. 2013; 11:Suppl 1. S120–S126.
Article24. Echternach M, Maurer CA, Mencke T, Schilling M, Verse T, Richter B. Laryngeal complications after thyroidectomy: is it always the surgeon? Arch Surg. 2009; 144:149–153.25. Goretzki PE, Schwarz K, Brinkmann J, Wirowski D, Lammers BJ. The impact of intraoperative neuromonitoring (IONM) on surgical strategy in bilateral thyroid diseases: is it worth the effort? World J Surg. 2010; 34:1274–1284.
Article26. Dralle H, Lorenz K, Schabram P, Musholt TJ, Dotzenrath C, Goretzki PE, et al. Intraoperative neuromonitoring in thyroid surgery. Recommendations of the Surgical Working Group for Endocrinology. Chirurg. 2013; 84:1049–1056.27. Dralle H, Schneider R, Lorenz K, Phuong NT, Sekulla C, Machens A. Vocal cord paralysis after thyroid surgery: current medicolegal aspects of intraoperative neuromonitoring. Chirurg. 2015; 86:698–706.28. Angelos P. Recurrent laryngeal nerve monitoring: state of the art, ethical and legal issues. Surg Clin North Am. 2009; 89:1157–1169.
Article29. Horne SK, Gal TJ, Brennan JA. Prevalence and patterns of intraoperative nerve monitoring for thyroidectomy. Otolaryngol Head Neck Surg. 2007; 136:952–956.
Article30. Sturgeon C, Sturgeon T, Angelos P. Neuromonitoring in thyroid surgery: attitudes, usage patterns, and predictors of use among endocrine surgeons. World J Surg. 2009; 33:417–425.
Article31. Timmermann W, Hamelmann WH, Thomusch O, Sekulla C, Grond S, Neumann HJ, et al. Effectiveness and results of intraoperative neuromonitoring in thyroid surgery. Statement of the Interdisciplinary Study Group on Intraoperative Neuromonitoring of Thyroid Surgery. Chirurg. 2004; 75:916–922.
Article32. Godballe C. Registry of surgical results: organization and outcomes. In : 34th Annual Meeting of the European Thyroid Association; 2009 Sep 5–9; Lisbon, Portugal. Altdorf: European Thyroid Association;2009.33. Dionigi G, Bacuzzi A, Boni L, Rausei S, Rovera F, Dionigi R. Visualization versus neuromonitoring of recurrent laryngeal nerves during thyroidectomy: what about the costs? World J Surg. 2012; 36:748–754.
Article34. Schneider R, Sekulla C, Machens A, Lorenz K, Nguyen Thanh P, Dralle H. Postoperative vocal fold palsy in patients undergoing thyroid surgery with continuous or intermittent nerve monitoring. Br J Surg. 2015; 102:1380–1387.
Article35. Lin YC, Dionigi G, Randolph GW, Lu IC, Chang PY, Tsai SY, et al. Electrophysiologic monitoring correlates of recurrent laryngeal nerve heat thermal injury in a porcine model. Laryngoscope. 2015; 125:E283–E290.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Neuromonitoring during Thyroid Surgery
- The Present and Future of Intraoperative Neuromonitoring in Thyroid Surgery
- Innovations in neuromonitoring and regenerative approaches in thyroid and neck surgeries
- Efficiency of Intraoperative Recurrent Laryngeal Nerve Monitoring Using Electromyography Tube in Reoperative Thyroid Surgery
- Precision and protection: advancements and future of neuromonitoring techniques for laryngeal surgery
