Korean J Gastroenterol.
2016 Nov;68(5):274-278. 10.4166/kjg.2016.68.5.274.
Acute Pancreatitis Complicated with Diabetic Ketoacidosis in a Young Adult without Hypertriglyceridemia: A Case Report
- Affiliations
-
- 1Department of Internal Medicine, CHA Gumi Medical Center, CHA University School of Medicine, Gumi, Korea. zenus1@hanmail.net
- KMID: 2383506
- DOI: http://doi.org/10.4166/kjg.2016.68.5.274
Abstract
- Systemic complications related to acute pancreatitis include acute respiratory distress syndrome, multiple organ dysfunction syndrome, disseminated intravascular coagulation, hypocalcemia, hyperglycemia, and insulin dependent diabetes or diabetic ketoacidosis. In practice, the development of diabetic ketoacidosis induced by acute pancreatitis is rare and generally associated with hypertriglyceridemia. However, herein we report a case of a 34-year-old female without hypertriglyceridemia, who was diagnosed with acute pancreatitis complicated with diabetic ketoacidosis. The patient was admitted with complaints of febrile sensation, back pain, and abdominal pain around the epigastric area. Levels of serum amylase and lipase were elevated to 663 U/L and 3,232 U/L. Contrast-enhanced abdominal CT showed pancreatic swelling, peri-pancreatic fat infiltration and fluid collection. The patient was initially diagnosed with simple acute pancreatitis. Though the symptoms were rapidly relieved after initiation of treatment, severe hyperglycemia (575 mg/dL), severe metabolic acidosis (pH 6.9), and ketonuria developed at four days after hospitalization. However, serum triglyceride levels remained within the normal range (134 mg/dL). Finally, the patient was diagnosed with acute pancreatitis complicated with diabetic ketoacidosis unrelated to hypertriglyceridemia. She recovered through insulin and fluid therapy, and receives insulin therapy at the outpatient clinic.
MeSH Terms
-
Abdominal Pain
Acidosis
Adult
Ambulatory Care Facilities
Amylases
Back Pain
Diabetic Ketoacidosis*
Disseminated Intravascular Coagulation
Female
Fluid Therapy
Hospitalization
Humans
Hyperglycemia
Hypertriglyceridemia*
Hypocalcemia
Insulin
Ketosis
Lipase
Multiple Organ Failure
Pancreatitis*
Reference Values
Respiratory Distress Syndrome, Adult
Sensation
Tomography, X-Ray Computed
Triglycerides
Young Adult*
Amylases
Insulin
Lipase
Figure
-
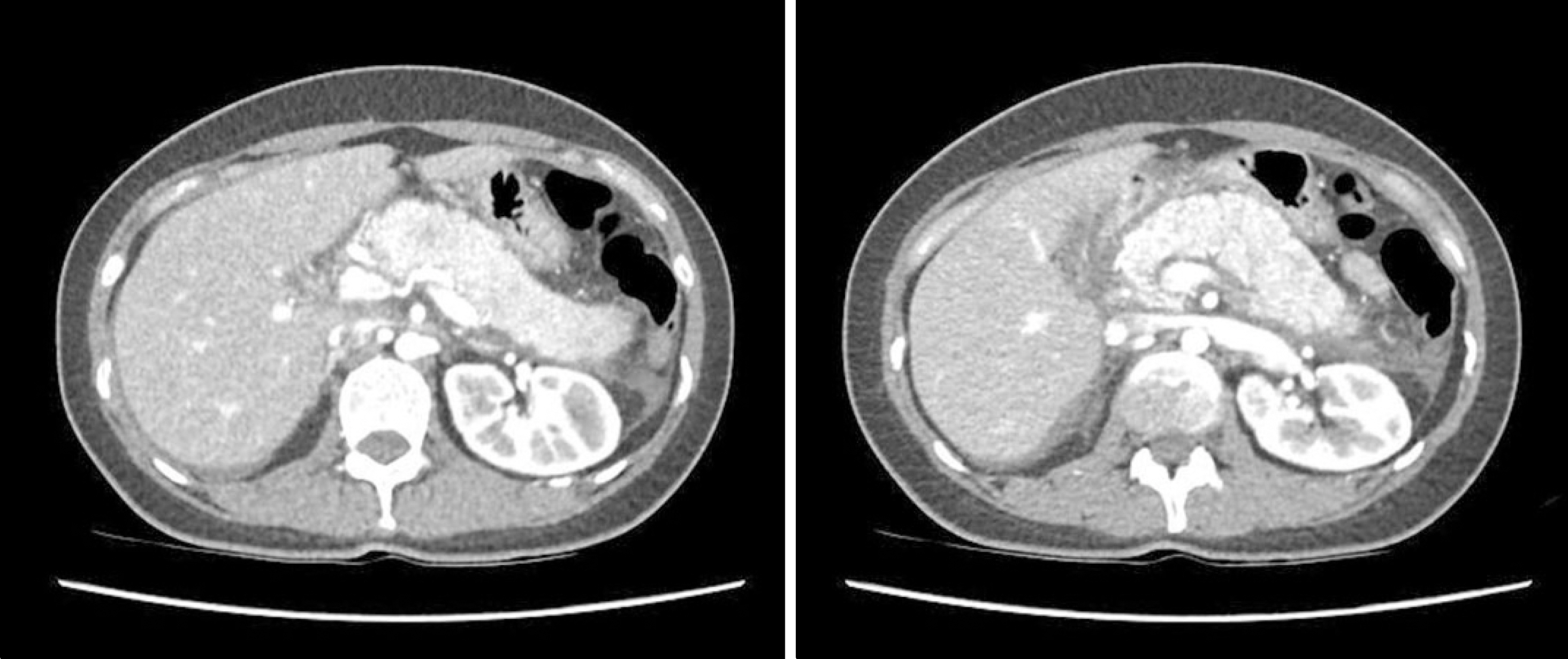
Fig. 1. Contrastenhanced abdominal CT scans at admission showed a diffuse edematous change of the pancreas, peripancreatic fat infiltration, and peripancreatic fluid collection.

Fig. 2. Contrastenhanced abdominal CT scans at the time of diagnosis of diabetic ketoacidosis revealed slightly swelling of the pancreas, and no evidence of necrosis and newly developed complications.

Fig. 3. Changes in the patient's arterial pH and serum glucose levels. HD, hospital day.
Reference
-
References
1. Steinberg W, Tenner S. Acute pancreatitis. N Engl J Med. 1994; 330:1198–1210.
Article2. Browne GW, Pitchumoni CS. Pathophysiology of pulmonary complications of acute pancreatitis. World J Gastroenterol. 2006; 12:7087–7096.
Article3. Aboulhosn K, Arnason T. Acute pancreatitis and severe hyper-triglyceridaemia masking unsuspected underlying diabetic ketoacidosis. BMJ Case Rep. 2013. DOI: doi:10.1136/bcr-2013–200431.
Article4. Quintanilla-Flores DL, Rendón-Ramírez EJ, Colunga-Pedraza PR, Gallardo-Escamilla J, Corral-Benavides SA, González-González JG, et al. Clinical course of diabetic ketoacidosis in hyper-triglyceridemic pancreatitis. Pancreas. 2015; 44:615–618.
Article5. Shenoy SD, Cody D, Rickett AB, Swift PG. Acute pancreatitis and its association with diabetes mellitus in children. J Pediatr Endocrinol Metab. 2004; 17:1667–1670.
Article6. Ranson JH, Rifkind KM, Roses DF, Fink SD, Eng K, Spencer FC. Prognostic signs and the role of operative management in acute pancreatitis. Surg Gynecol Obstet. 1974; 139:69–81.7. Johnson CD, Toh SK, Campbell MJ. Combination of APACHE-II score and an obesity score (APACHE-O) for the prediction of severe acute pancreatitis. Pancreatology. 2004; 4:1–6.
Article8. Balthazar EJ. CT diagnosis and staging of acute pancreatitis. Radiol Clin North Am. 1989; 27:19–37.9. Lankisch PG, Apte M, Banks PA. Acute pancreatitis. Lancet. 2015; 386:85–96.
Article10. Johnson CD, Besselink MG, Carter R. Acute pancreatitis. BMJ. 2014; 349:g4859.
Article11. Singla AA, Ting F, Singla A. Acute pancreatitis secondary to diabetic ketoacidosis induced hypertriglyceridemia in a young adult with undiagnosed type 2 diabetes. JOP. 2015; 16:201–204.12. Nair S, Yadav D, Pitchumoni CS. Association of diabetic ketoacidosis and acute pancreatitis: observations in 100 consecutive episodes of DKA. Am J Gastroenterol. 2000; 95:2795–2800.
Article13. Nair S, Pitchumoni CS. Diabetic ketoacidosis, hyperlipidemia, and acute pancreatitis: the enigmatic triangle. Am J Gastroenterol. 1997; 92:1560–1561.14. Winter RJ, Herr TJ, Stone NJ, Traisman HS. Diabetic lipemia in childhood diabetic ketoacidosis: a clue to coexisting acute pancreatitis. Diabetes Care. 1980; 3:706–767.
Article15. Hahn SJ, Park JH, Lee JH, Lee JK, Kim KA. Severe hypertriglyceridemia in diabetic ketoacidosis accompanied by acute pancreatitis: case report. J Korean Med Sci. 2010; 25:1375–1378.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Severe Hypertriglyceridemia in Diabetic Ketoacidosis Accompanied by Acute Pancreatitis: Case Report
- Ketoacidosis with Hypertriglyceridemia-Induced Pancreatitis in a Patient with Gestational Diabetes: A Case Report
- Concurrent Diabetic Ketoacidosis and Acute Pancreatitis in Mild Hypertriglyceridemia: An Enigmatic Triangle
- Cheese-like Material in the Heart: An Autopsy Case Report of Severe Hypertriglyceridemia in Diabetic Ketoacidosis Patient
- A case of acute pancreatitis induced by hypertriglyceridemia in gestational diabetes
