A Case of a Corneal Stromal Penetrating Injury via an Ejected Needle during Stromal Hydration
- Affiliations
-
- 1Department of Ophthalmology, Dankook University College of Medicine, Cheonan, Korea. persica79@naver.com
- KMID: 2382683
- DOI: http://doi.org/10.3341/jkos.2017.58.6.725
Abstract
- PURPOSE
We report a case of a horizontally penetrating injury of corneal stroma via an ejected irrigating needle during stromal hydration in cataract surgery.
CASE SUMMARY
A 79-year-old woman presented with decreased visual acuity in her right eye. Her best corrected visual acuity in the right eye was 0.3. The cataract score of her right eye was nuclear opacity 3, cortical opacity 1−2, and posterior subcapsular opacity 1. She underwent phacoemulsification using a clear corneal approach while under topical anesthesia, and an intraocular lens was successfully implanted in the bag. A plastic syringe with an irrigating needle was used to hydrate the corneal stroma at the clear cornea site. As a result of the increased pressure applied to the connection between the syringe and irrigating needle, the loosened irrigating needle was forcefully ejected toward the corneal endothelium, horizontally penetrating the stroma without injuring the corneal epithelium. On the 1st postoperative day, her right eye exhibited a visual acuity of 0.5, astigmatism of −1.25 diopter (D) cyl., corneal edema with Descemet's folds, and insignificant scarring of the corneal endothelium. Three weeks after surgery, the visual acuity was 0.9, the astigmatism was −0.50 D, and any other abnormalities such as corneal opacity were no longer present.
CONCLUSIONS
Despite a penetrating needle injury through the corneal endothelium and stroma, the corneal wound healing process did not result in corneal opacity or worsened astigmatism. To prevent sequela due to an ejected irrigating needle, operators and assistants should be actively aware of tight locking between the needle and syringe.
MeSH Terms
Figure
-
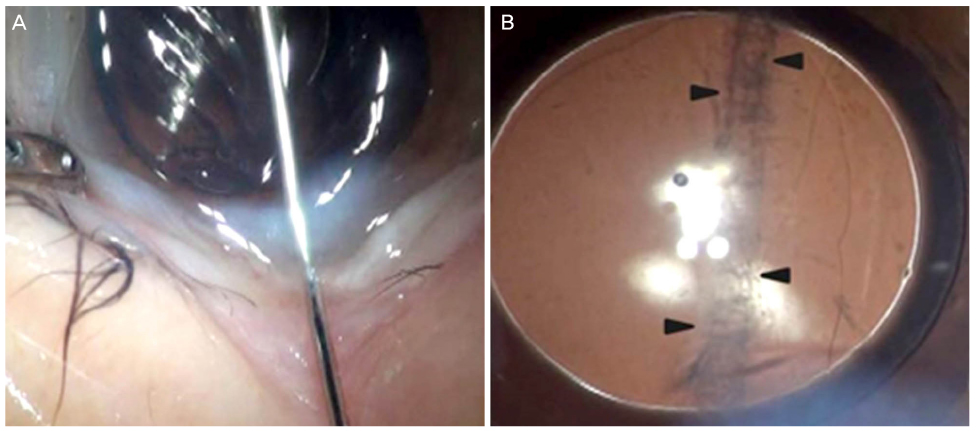
Figure 1 In process of hydration of corneal stroma during cataract surgery, the loosed irrigating needle was ejected. (A) The 27 gauge needle penetrated through the corneal stroma horizontally from the 9 o'clock clear cornea incision site. (B) After removing the needle, the linear wound remained across the corneal stroma (arrowheads).

Figure 2 On the 1st postoperative day, the cornea was edematous and Descemet's membrane folds were detected. (A) The stromal linear wound was remarkably healed compared to that of the operation day, and (B) the opacity of endothelium was at the around center of the cornea (arrowheads). Anterior segment optical coherence tomography showed (C) linear wound of stroma and (D) minimal enlargement of stroma with detachment of Descemet's membrane (arrowheads).
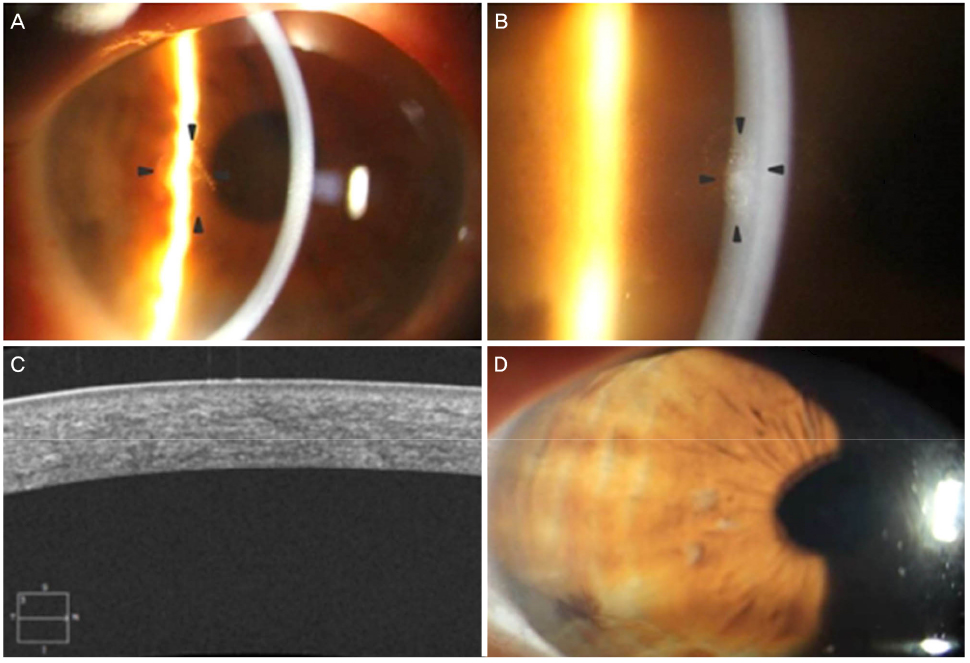
Figure 3 On the 6th postoperative day, corneal edema and Descemet's membrane folds were greatly improved. (A) Stromal lesion was almost disappeared and (B) endothelial opacity was also nearly faded (arrowheads). About 3 weeks after surgery, visual acuity of affected eye was 0.9 and astigmatism wasn't induced by the penetrating injury. (C) No corneal opacity remained and (D) rebuilding process of corneal stroma, Descemet's membrane and endothelium was fairly successful without any sequela.
Reference
-
1. Yoon SC, Jung JW, Sohn HJ, Shyn KH. Cataract and refractive surgery in; a survey of KSCRS members from 1995~2006. Korean J Ophthalmol. 2009; 23:142–147.2. Rumelt S, Kassif Y, Koropov M, et al. The spectrum of iatrogenic intraocular injuries caused by inadvertent cannula release during anterior segment surgery. Arch Ophthalmol. 2007; 125:889–892.3. Prenner JL, Tolentino MJ, Maguire AM. Traumatic retinal break from viscoelastic cannula during cataract surgery. Arch Ophthalmol. 2003; 121:128–129.4. Munshi V, Sampat V, Pagliarini S. Zonular dialysis and vitreous loss with a J-shaped hydrodissection cannula during phacoemulsification. J Cataract Refract Surg. 2005; 31:450–451.5. Saha N, Price NC. Iatrogenic retinal tear and vitreous hemorrhage with Rycroft cannula during phacoemulsification cataract surgery. Eye. 2003; 17:260–261.6. Wiggins MN, Uwaydat SH. Cannula ejection into the cornea during wound hydration. Br J Ophthalmol. 2008; 92:181.7. Reinstein DZ, Archer TJ, Gobbe M, et al. Epithelial thickness in the normal cornea: three-dimensional display with Artemis very high-frequency digital ultrasound. J Refract Surg. 2008; 24:571–581.8. Dohlman CH. The function of the corneal epithelium in health and disease. The Jonas S. Friedenwald Memorial Lecture. Invest Ophthalmol. 1971; 10:383–407.9. Zagon IS, Sassani JW, Ruth TB, McLaughlin PJ. Epithelial adhesion complexes and organ culture of the human cornea. Brain Res. 2001; 900:205–213.10. Taylor RJ, Wang MX. Rate of re-epithelialization following amniotic membrane transplantation. Invest Ophthalmol Vis Sci. 1998; 39:S1038.11. Meller D, Pires RT, Mack RJ, et al. Amniotic membrane transplantation for acute chemical or thermal burns. Ophthalmology. 2000; 107:980–989.12. Kruse FE, Rohrschneider K, Völcker HE. Multilayer amniotic membrane transplantation for reconstruction of deep corneal ulcers. Ophthalmology. 1999; 106:1504–1511.13. Chen HJ, Pires RT, Tseng SC. Amniotic membrane transplantation for severe neurotrophic corneal ulcers. Br J Ophthalmol. 2000; 84:826–833.14. Kim JS, Kim JC, Hahn TW, Park WC. Amniotic membrane transplantation in infectious corneal ulcer. Cornea. 2001; 20:720–726.15. Solomon A, Pires RT, Tseng SC. Amniotic membrane transplantation after extensive removal of primary and recurrent pterygia. Ophthalmology. 2001; 108:449–460.16. Hanada K, Shimazaki J, Shimmura S, Tsubota K. Multilayered amniotic membrane transplantation for severe ulceration of the cornea and sclera. Am J Ophthalmol. 2001; 131:324–331.17. Labat-Robert J, Robert L. Fifty years of structural glycoproteins. Pathol Biol (Paris). 2012; 60:66–75.18. Bourne WM. Clinical estimation of corneal endothelial pump function. Trans Am Ophthalmol Soc. 1998; 96:229–239. discussion 239-42.19. Riley MV, Winkler BS, Starnes CA, et al. Regulation of corneal endothelial barrier function by adenosine, cyclic AMP, and protein kinases. Invest Ophthalmol Vis Sci. 1998; 39:2076–2084.20. Wang L, Dixit L, Weikert MP, et al. Healing change in clear corneal cataract incisions evaluated using Fourier-domain optical coherence tomography. J Cataract Refract Surg. 2012; 38:660–665.21. Asano-Kato N, Toda I, Hori-Komai Y, et al. Epithelial ingrowth after laser in situ keratomileusis: clinical features and possible mechanisms. Am J Ophthalmol. 2002; 134:801–807.22. Kong HY, Ko IH, Lee JB. Comparison of laser epithelial keratomileusis (LASEK) in one eye and photorefractive keratectomy (PRK) in other eye for low to moderate myopia. J Korean Ophthalmol Soc. 2001; 42:825–831.23. Melles GR, Ong TS, Ververs B, van der Wees J. Descemet membrane endothelial keratoplasty (DMEK). Cornea. 2006; 25:987–990.24. Rudolph M, Laaser K, Bachmann BO, et al. Corneal higher-order aberrations after Descemet's membrane endothelial keratoplasty. Ophthalmology. 2012; 119:528–535.25. Gupta D, Burton B, Goldsmith C, et al. Iatrogenic retinal detachment due to canuula slippage despite use of luer-lock syringe system. J Cataract Refract Surg. 2008; 34:1612.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Effect of Amniotic Membrane Graft on the Inhibition of Corneal Opacity After Traumatic Injury
- Structural Analysis of Different Incision Sizes and Stromal Hydration in Cataract Surgery Using Anterior Segment Optical Coherence Tomography
- Two Cases of Congenital Hereditary Stromal Dystrophy of the Cornea
- Interactions of Corneal Endothelial Cells with Stromal Cells during Corneal Endothelial Injury
- Anterior Stromal Puncture with 26-Gauge Needle for Recurrent Corneal Erosion: A Report of Five Cases
