Korean J Sports Med.
2016 Dec;34(2):127-131. 10.5763/kjsm.2016.34.2.127.
Morphologic Analysis of the Fifth Metatarsal Stress Fracture: The Precise Coronal and Sagittal Location
- Affiliations
-
- 1Foot and Ankle Service, KT Lee's Orthopedic Hospital, Seoul, Korea.
- 2Foot and Ankle Clinic, Department of Orthopedic Surgery, Eulji Medical Center, Eulji University School of Medicine, Seoul, Korea.
- 3Department of Orthopedic Surgery, Ajou University Hospital, Ajou University School of Medicine, Suwon, Korea. parkyounguk@gmail.com
- KMID: 2382049
- DOI: http://doi.org/10.5763/kjsm.2016.34.2.127
Abstract
- From a biomechanical standpoint, the main pathologic abnormality of fifth metatarsal stress fracture is the location where repetitive tensile stress concentrated. Decreasing tensile force in this region would be a proper treatment. Therefore, the purpose of this study is to evaluate the precise sagittal and coronal location of the fifth metatarsal stress fracture. Between June 2012 and May 2013, 38 athletes with a fifth metatarsal stress fracture were treated. To evaluate the precise sagittal location of the fracture, the entire length of the fifth metatarsal was measured and the distance from tuberosity to the fracture line was measured. To evaluate the precise coronal location of the fractures, coronal computed tomography images were obtained for incomplete fracture cases. The fracture location was classified as four quadrants. Thirty patients were classified into zone III fracture. However, the fracture is located in zone II for remaining eight cases. The median value of ratio between whole length and the distance from tuberosity to the fracture was 0.35 (range, 0.29-0.40) Among 33 incomplete fracture cases, there were 28 patients whose fracture developed in plantolateral quadrant, four patients at the lateral side and a patient for plantar side. The main pathologic abnormality is at the plantar lateral side because of the repetitive stress concentrated there.
Keyword
Figure
-
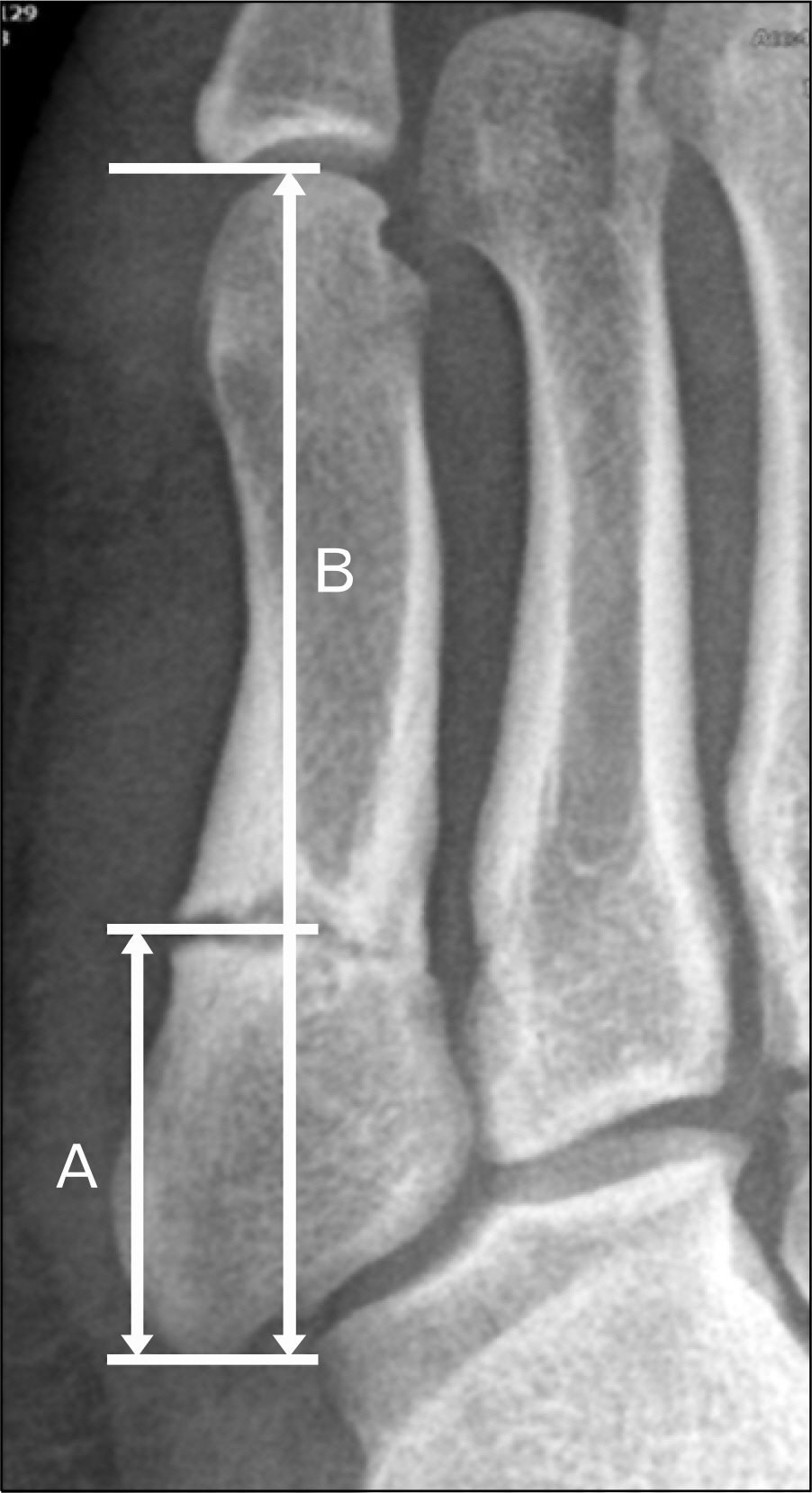
Fig. 1. The entire length of the fifth metatarsal was measured on a 30-degree internal oblique view. The distance from tuberosity to the fracture line was measured. The ratio between the entire length and the distance from tuberosity to the fracture (A, B) were calculated.
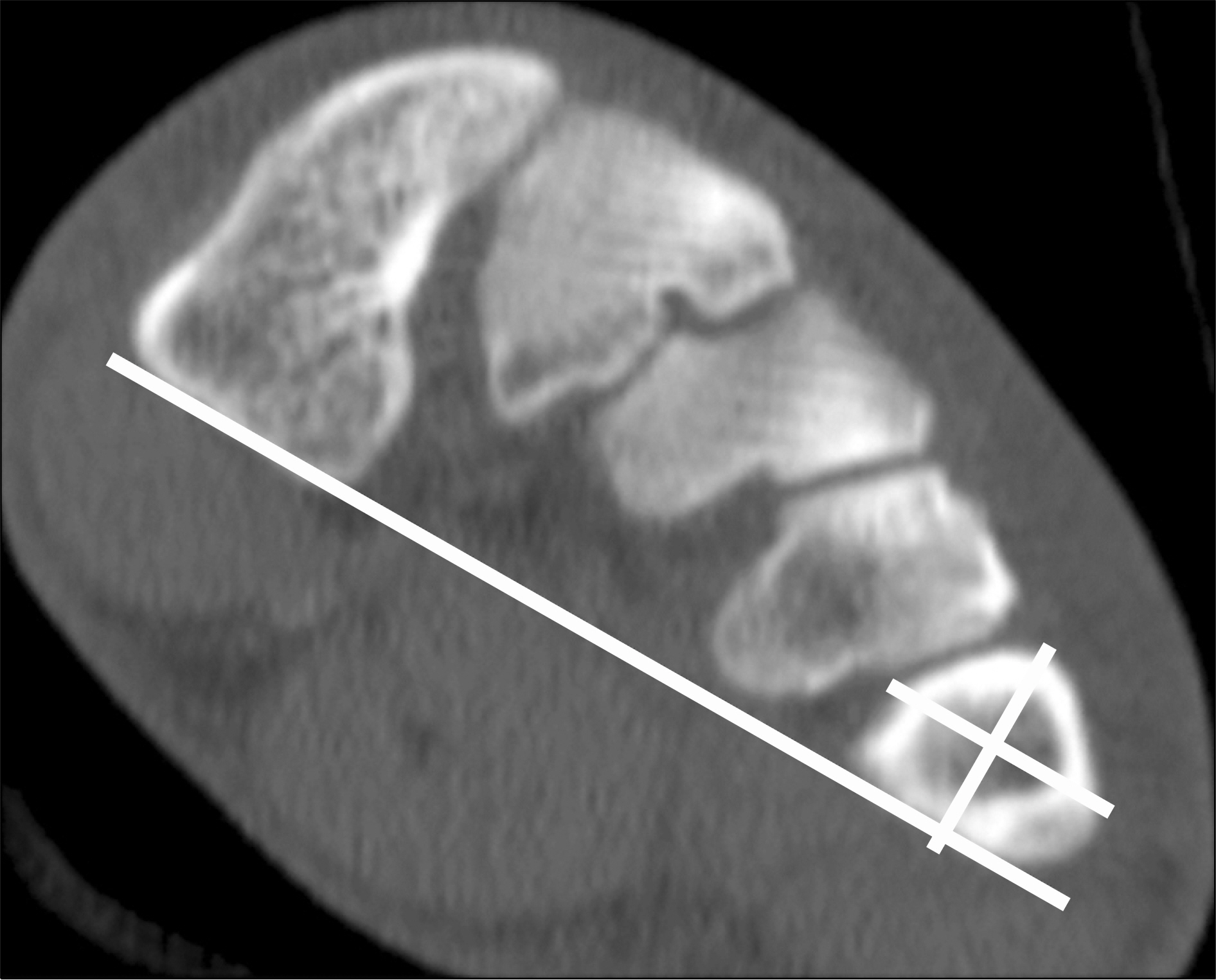
Fig. 2. The fracture location was classified into four quadrants: dorsomedial, dorsolateral, plantomedial, and plan-tolateral. The quadrant was made as a reference to the line formed between the most inferior margin of the first metatarsal and the fifth metatarsal. The second line was drawn parallel to this line centered to the fifth metatarsal center. The third line was drawn perpendicular to the second line centered to the fifth metatarsal.
Reference
-
References
1. Jones R. I: fracture of the base of the fifth metatarsal bone by indirect violence. Ann Surg. 1902; 35:697–700.2. Quill GE Jr. Fractures of the proximal fifth metatarsal. Orthop Clin North Am. 1995; 26:353–61.
Article3. Zwitser EW, Breederveld RS. Fractures of the fifth metatarsal; diagnosis and treatment. Injury. 2010; 41:555–62.
Article4. Lee KT, Park YU, Young KW, Kim JS, Kim JB. The plantar gap: another prognostic factor for fifth metatarsal stress fracture. Am J Sports Med. 2011; 39:2206–11.5. Lee KT, Park YU, Jegal H, Park JW, Choi JP, Kim JS. Prognostic classification of fifth metatarsal stress fracture using plantar gap. Foot Ankle Int. 2013; 34:691–6.
Article6. Lee KT, Young KW, Park SY, Lee YK, Na SE. Surgical results of 5th metatarsal stress fracture using two cortical screws and wire determining of time of return to full sports activity in soccer players. Korean J Sports Med. 2009; 27:14–8.7. Magnan B, Bragantini A, Regis D, Bartolozzi P. Metatarsal lengthening by callotasis during the growth phase. J Bone Joint Surg Br. 1995; 77:602–7.
Article8. Torg JS, Balduini FC, Zelko RR, Pavlov H, Peff TC, Das M. Fractures of the base of the fifth metatarsal distal to the tuberosity: classification and guidelines for nonsurgical and surgical management. J Bone Joint Surg Am. 1984; 66:209–14.
Article9. Lawrence SJ, Botte MJ. Jones' fractures and related fractures of the proximal fifth metatarsal. Foot Ankle. 1993; 14:358–65.
Article10. Dameron TB Jr. Fractures and anatomical variations of the proximal portion of the fifth metatarsal. J Bone Joint Surg Am. 1975; 57:788–92.
Article11. Rosenberg GA, Sferra JJ. Treatment strategies for acute fractures and nonunions of the proximal fifth metatarsal. J Am Acad Orthop Surg. 2000; 8:332–8.
Article12. Dameron TB Jr. Fractures of the proximal fifth metatarsal: selecting the best treatment option. J Am Acad Orthop Surg. 1995; 3:110–4.
Article13. Polzer H, Polzer S, Mutschler W, Prall WC. Acute fractures to the proximal fifth metatarsal bone: development of classification and treatment recommendations based on the current evidence. Injury. 2012; 43:1626–32.
Article14. Chuckpaiwong B, Queen RM, Easley ME, Nunley JA. Distinguishing Jones and proximal diaphyseal fractures of the fifth metatarsal. Clin Orthop Relat Res. 2008; 466:1966–70.
Article15. Carp L. Fracture of the fifth metatarsal bone: with special reference to delayed union. Ann Surg. 1927; 86:308–20.
Article16. Clapper MF, O'Brien TJ, Lyons PM. Fractures of the fifth metatarsal: analysis of a fracture registry. Clin Orthop Relat Res. 1995; 315:238–41.17. DeLee JC, Evans JP, Julian J. Stress fracture of the fifth metatarsal. Am J Sports Med. 1983; 11:349–53.
Article18. Hatch RL, Alsobrook JA, Clugston JR. Diagnosis and management of metatarsal fractures. Am Fam Physician. 2007; 76:817–26.19. Hens J, Martens M. Surgical treatment of Jones fractures. Arch Orthop Trauma Surg. 1990; 109:277–9.
Article20. Hulkko A, Orava S, Nikula P. Stress fracture of the fifth metatarsal in athletes. Ann Chir Gynaecol. 1985; 74:233–8.21. Zelko RR, Torg JS, Rachun A. Proximal diaphyseal fractures of the fifth metatarsal: treatment of the fractures and their complications in athletes. Am J Sports Med. 1979; 7:95–101.
Article22. Kavanaugh JH, Brower TD, Mann RV. The Jones fracture revisited. J Bone Joint Surg Am. 1978; 60:776–82.
Article23. Glasgow MT, Naranja RJ Jr, Glasgow SG, Torg JS. Analysis of failed surgical management of fractures of the base of the fifth metatarsal distal to the tuberosity: the Jones fracture. Foot Ankle Int. 1996; 17:449–57.
Article24. Hunt KJ, Anderson RB. Treatment of Jones fracture nonunions and refractures in the elite athlete: outcomes of intramedullary screw fixation with bone grafting. Am J Sports Med. 2011; 39:1948–54.25. Josefsson PO, Karlsson M, Redlund-Johnell I, Wendeberg B. Jones fracture: surgical versus nonsurgical treatment. Clin Orthop Relat Res. 1994; 299:252–5.
Article26. Wright RW, Fischer DA, Shively RA, Heidt RS Jr, Nuber GW. Refracture of proximal fifth metatarsal (Jones) fracture after intramedullary screw fixation in athletes. Am J Sports Med. 2000; 28:732–6.27. Mindrebo N, Shelbourne KD, Van Meter CD, Rettig AC. Outpatient percutaneous screw fixation of the acute Jones fracture. Am J Sports Med. 1993; 21:720–3.
Article28. Sarimo J, Rantanen J, Orava S, Alanen J. Tension-band wiring for fractures of the fifth metatarsal located in the junction of the proximal metaphysis and diaphysis. Am J Sports Med. 2006; 34:476–80.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stress Fracture on the 4th Metatarsal Bone after Treatment of Stress Fracture on the 5th Metatarsal Bone: A Case Report
- The Fatigue Fracture of the Metatarsal in an Unilateral A-K amputee: A case report
- The Relationship between Stud Morphology and 5th Metatarsal Proximal Stress Fractures on Soccer Players
- Morphometrics of the Metatarsal Bone and Regression Equation of the Metatarsal Length in Korean
- Medial Malleolar Stress Fracture in Athlete
