Orbital Lymphangioma: Characteristics and Treatment Outcomes of 12 Cases
- Affiliations
-
- 1Institute of Vision Research, Department of Ophthalmology, Yonsei University College of Medicine, Seoul, Korea. yoonjs@yuhs.ac
- 2Department of Ophthalmology, Saint John's Episcopal Hospital, Far Rockaway, NY, USA.
- KMID: 2379875
- DOI: http://doi.org/10.3341/kjo.2016.0034
Abstract
- PURPOSE
To report the patient characteristics and treatment outcomes in 12 cases of orbital lymphangioma.
METHODS
In this study, orbital lymphangioma was diagnosed based on clinical, radiologic (computed tomography, magnetic resonance imaging), and histologic findings when possible. Patients whose vision was not compromised by orbital lymphangioma, or that did not have increased intraocular pressure (IOP), received oral corticosteroids. Orbital lymphangioma that affected vision or increased IOP was treated by surgery, which included aspiration of blood or partial resection with or without injection of a sclerosant.
RESULTS
Four patients without compromised vision responded well to oral corticosteroids. Eight patients with compromised vision underwent some form of surgery. Bleeding recurred in three patients after aspiration of blood and in two after partial resection and intralesional injection of a sclerosant. Overall, five patients were treated successfully by aspiration of blood, intralesional injection of a sclerosant, and application of continuous negative pressure by appropriate drainage. Partial resection was successful in two patients with organized hematoma.
CONCLUSIONS
Orbital lymphangioma that does not compromise vision can be treated medically using oral corticosteroids. Patients with threatened vision or elevated IOP due to acute hemorrhage should be treated by aspiration of blood, intralesional injection of a sclerosant, and application of continuous negative pressure. Partial resection may be effective only in patients with organized hematoma.
Keyword
MeSH Terms
Figure
-
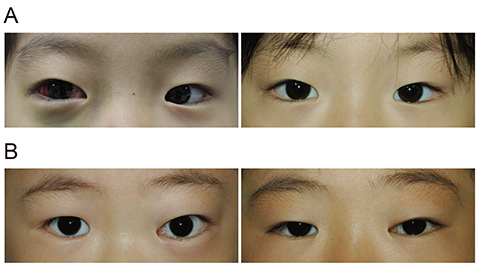
Fig. 1 Patients with orbital lymphangioma that were successfully treated with oral corticosteroids. (A) Case 6, (B) case 8 (left column, pretreatment; right column, posttreatment).
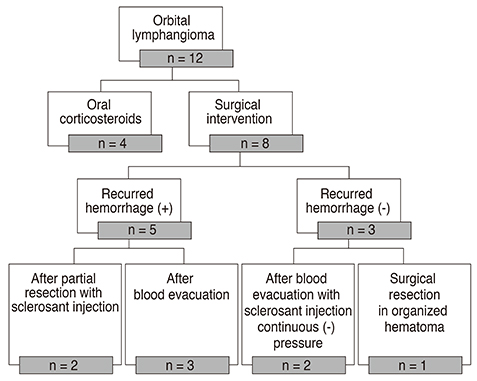
Fig. 2 Treatment modalities of patients with orbital lymphangioma who underwent surgical intervention and experienced recurrent hemorrhage.
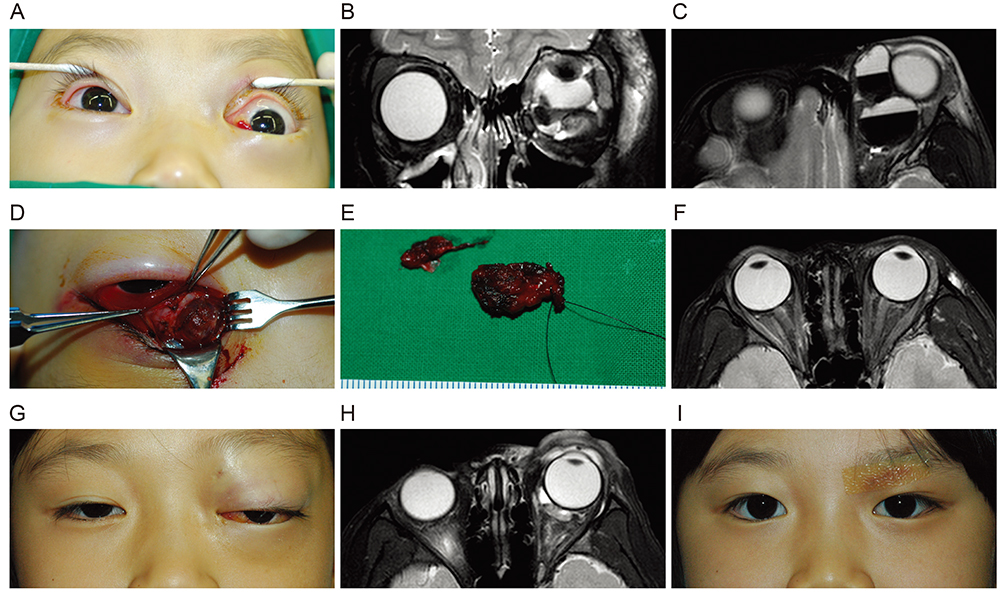
Fig. 3 Four-year-old girl with left orbital lymphangioma. (A) Proptosis at initial visit. (B) Axial T2-weighted magnetic resonance image showing multiple diffusely-infiltrating cysts. (C) Coronal T2-weighted magnetic resonance image showing cysts with fluid-fluid levels. (D) Lymphangioma observed via the anterior orbitotomy site. (E) Partially-resected lymphangioma. (F) Axial T2-weighted magnetic resonance image showing that the cystic mass had been removed from the left orbit. (G) Bleeding recurred 30 months after the first surgical intervention. (H) Axial T2-weighted magnetic resonance image indicating bleeding from deep residual lymphangiomatous tissue. (I) Appearance 6 months after the repeated surgery; bleeding has not recurred, but the patient's visual acuity has changed to no light perception.

Fig. 4 Nineteen-year-old man with a 16-year history of left orbital lymphangioma. (A) Severe proptosis and conjunctival swelling before resection. (B) Exophthalmometry showing 35-mm protrusion of the left eyeball. (C) Coronal T2-weighted magnetic resonance image showing lymphangioma that occupied most of the left orbit. (D) Axial T2-weighted magnetic resonance image showing a large lymphangioma with organized hematoma anteriorly displacing the left eyeball. (E) Reduced proptosis after partial resection. (F) Computed tomography image after partial resection.
Reference
-
1. Guinto G, Guinto-Nishimura Y. Orbital lymphangiomas. World Neurosurg. 2014; 81:708–709.2. Rootman J, Hay E, Graeb D, Miller R. Orbital-adnexal lymphangiomas: a spectrum of hemodynamically isolated vascular hamartomas. Ophthalmology. 1986; 93:1558–1570.3. Russin JJ, Rangel-Castilla L, Kalani MY, Spetzler RF. Surgical management, outcomes, and recurrence rate of orbital lymphangiomas. J Clin Neurosci. 2015; 22:877–882.4. Lee KH, Han SH, Yoon JS. Successful treatment of orbital lymphangioma with intralesional bleomycin and application of continuous negative pressure. Korean J Ophthalmol. 2015; 29:70–72.5. Saha K, Leatherbarrow B. Orbital lymphangiomas: a review of management strategies. Curr Opin Ophthalmol. 2012; 23:433–438.6. Boulos PR, Harissi-Dagher M, Kavalec C, et al. Intralesional injection of Tisseel fibrin glue for resection of lymphangiomas and other thin-walled orbital cysts. Ophthal Plast Reconstr Surg. 2005; 21:171–176.7. Gandhi NG, Lin LK, O'Hara M. Sildenafil for pediatric orbital lymphangioma. JAMA Ophthalmol. 2013; 131:1228–1230.8. Tunc M, Sadri E, Char DH. Orbital lymphangioma: an analysis of 26 patients. Br J Ophthalmol. 1999; 83:76–80.9. Jastrzebski A, Brownstein S, Manusow J, Rubab S. Isolated conjunctival lymphangioma. Can J Ophthalmol. 2011; 46:369–370.10. Haik BG, Saint Louis L, Smith ME, et al. Magnetic resonance imaging of orbital lymphangiomas. Am J Ophthalmol. 1987; 103:724–725.11. Kazim M, Kennerdell JS, Rothfus W, Marquardt M. Orbital lymphangioma: correlation of magnetic resonance images and intraoperative findings. Ophthalmology. 1992; 99:1588–1594.12. Bisdorff A, Mulliken JB, Carrico J, et al. Intracranial vascular anomalies in patients with periorbital lymphatic and lymphaticovenous malformations. AJNR Am J Neuroradiol. 2007; 28:335–341.13. Bond JB, Haik BG, Taveras JL, et al. Magnetic resonance imaging of orbital lymphangioma with and without gadolinium contrast enhancement. Ophthalmology. 1992; 99:1318–1324.14. Graeb DA, Rootman J, Robertson WD, et al. Orbital lymphangiomas: clinical, radiologic, and pathologic characteristics. Radiology. 1990; 175:417–421.15. Harris GJ, Sakol PJ, Bonavolonta G, De Conciliis C. An analysis of thirty cases of orbital lymphangioma: pathophysiologic considerations and management recommendations. Ophthalmology. 1990; 97:1583–1592.16. Wilson ME, Parker PL, Chavis RM. Conservative management of childhood orbital lymphangioma. Ophthalmology. 1989; 96:484–489.17. Wiegand S, Eivazi B, Zimmermann AP, et al. Sclerotherapy of lymphangiomas of the head and neck. Head Neck. 2011; 33:1649–1655.18. Gochi A, Orita K, Fuchimoto S, et al. The prognostic advantage of preoperative intratumoral injection of OK-432 for gastric cancer patients. Br J Cancer. 2001; 84:443–451.19. Katano M, Morisaki T. The past, the present and future of the OK-432 therapy for patients with malignant effusions. Anticancer Res. 1998; 18:3917–3925.20. Giguere CM, Bauman NM, Sato Y, et al. Treatment of lymphangiomas with OK-432 (Picibanil) sclerotherapy: a prospective multi-institutional trial. Arch Otolaryngol Head Neck Surg. 2002; 128:1137–1144.21. Suzuki Y, Obana A, Gohto Y, et al. Management of orbital lymphangioma using intralesional injection of OK-432. Br J Ophthalmol. 2000; 84:614–617.22. Yoon JS, Choi JB, Kim SJ, Lee SY. Intralesional injection of OK-432 for vision-threatening orbital lymphangioma. Graefes Arch Clin Exp Ophthalmol. 2007; 245:1031–1035.23. Saitta P, Krishnamurthy K, Brown LH. Bleomycin in dermatology: a review of intralesional applications. Dermatol Surg. 2008; 34:1299–1313.24. Muir T, Kirsten M, Fourie P, et al. Intralesional bleomycin injection (IBI) treatment for haemangiomas and congenital vascular malformations. Pediatr Surg Int. 2004; 19:766–773.25. Gooding C, Meyer D. Intralesional bleomycin: a potential treatment for refractory orbital lymphangiomas. Ophthal Plast Reconstr Surg. 2014; 30:e65–e67.26. Swetman GL, Berk DR, Vasanawala SS, et al. Sildenafil for severe lymphatic malformations. N Engl J Med. 2012; 366:384–386.27. Portnow LH, Scott M, Morris CG, et al. Fractionated radiotherapy in the management of benign vascular tumors. Am J Clin Oncol. 2012; 35:557–561.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case Report: Treatment of Orbital Lymphangioma with Intralesional OK-432 Injection
- Treatment of the orbital dystopia associated with cavernous lymphangioma
- Orbital Cavernous Lymphangioma with Intracranial Extension: Case Report
- Vaporization of Orbital Lymphangioma with Ultrapulse CO2 Laser
- Lymphangioma
