Restor Dent Endod.
2017 May;42(2):146-151. 10.5395/rde.2017.42.2.146.
Dental management of patients with X-linked hypophosphatemia
- Affiliations
-
- 1Department of Conservative Dentistry, School of Dentistry and Dental Science Research Institute, Chonnam National University, Gwangju, Korea. wmoh@chonnam.ac.kr
- KMID: 2379465
- DOI: http://doi.org/10.5395/rde.2017.42.2.146
Abstract
- X-linked hypophosphatemia (XLH) is a hereditary metabolic disease caused by the loss of phosphate through the renal tubules into the urine, and an associated decrease in serum calcium and potassium phosphate. Its dental features include spontaneous dental abscesses that occur in the absence of trauma or dental caries. The aim of this case report was to describe the dental problems of XLH patients and to evaluate limitations in their treatment. A 14 year old male and a 38 year old female with XLH were referred to the Department of Conservative Dentistry for endodontic treatment. The dental findings were periapical abscesses without obvious trauma or caries. Conservative endodontic treatment was performed in teeth with pulp necrosis and abscess. In case 1, the treated teeth showed improvements in bone healing, without clinical symptoms. However, in case 2, the implants and the treated tooth showed hypermobility, and the final restoration was therefore postponed. Early diagnosis, periodic examinations, and communication with the patient's pediatrician are important in the dental management of patients with XLH.
MeSH Terms
Figure
-
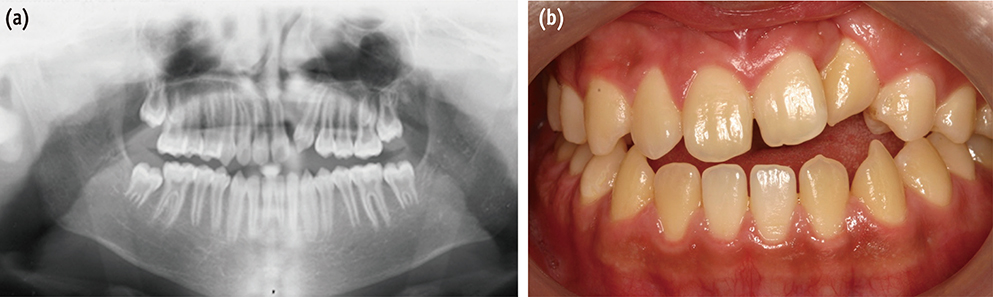
Figure 1 Preoperative panoramic view (a) and clinical photograph (b) of the patient in case 1.
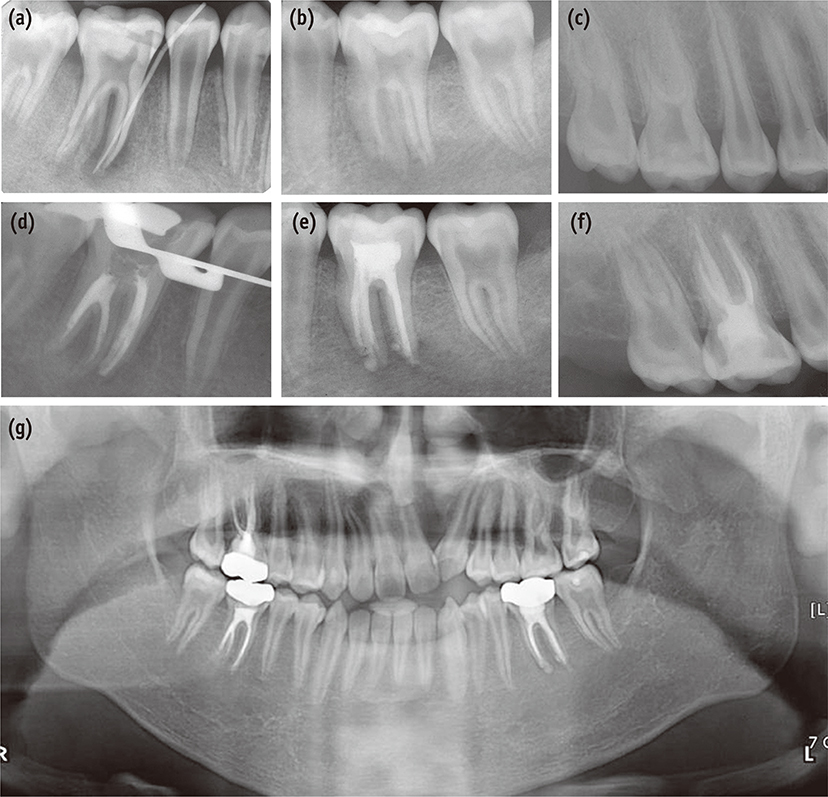
Figure 2 Radiographs of the patient in case 1. Preoperative (a) and postoperative (d) radiographs of the lower right first molar. Preoperative (b) and postoperative (e) radiographs of the lower left first molar. Preoperative (c) and postoperative (f) radiographs of the upper right first molar. Postoperative panoramic view (g).
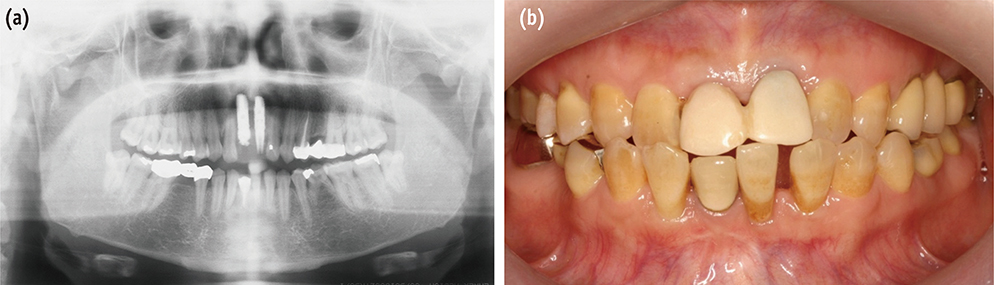
Figure 3 Preoperative panoramic view (a) and clinical photograph (b) of the patient in case 2.
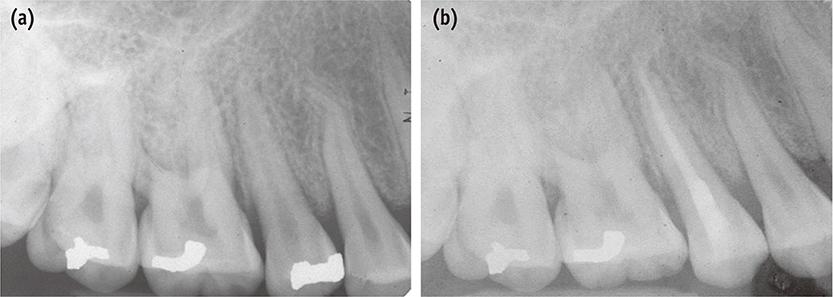
Figure 4 Radiographs of the patient in case 2. Preoperative (a) and postoperative (b) radiographs of the upper right second premolar.
Reference
-
1. Moreland LW. Rheumatology and immunology therapy (A to Z essentials): hypophosphatemic vitamin D resistant rickets. Springer;2004. p. 428.2. Beltes C, Zachou E. Endodontic management in a patient with vitamin D-resistant rickets. J Endod. 2012; 38:255–258.
Article3. Souza MA, Soares Junior LA, Santos MA, Vaisbich MH. Dental abnormalities and oral health in patients with Hypophosphatemic rickets. Clinics(Sao Paulo). 2010; 65:1023–1026.
Article4. Pereira CM, de Andrade CR, Vargas PA, Coletta RD, de Almeida OP, Lopes MA. Dental alterations associated with X-linked hypophosphatemic rickets. J Endod. 2004; 30:241–245.
Article5. Thomas MK, Demay MB. Vitamin D deficiency and disorders of vitamin D metabolism. Endocrinol Metab Clin North Am. 2000; 29:611–627.
Article6. Feng JQ, Clinkenbeard EL, Yuan B, White KE, Drezner MK. Osteocyte regulation of phosphate homeostasis and bone mineralization underlies the pathophysiology of the heritable disorders of rickets and osteomalacia. Bone. 2013; 54:213–221.
Article7. Koehne T, Marshall RP, Jeschke A, Kahl-Nieke B, Schinke T, Amling M. Osteopetrosis, osteopetrorickets and hypophosphatemic rickets differentially affect dentin and enamel mineralization. Bone. 2013; 53:25–33.
Article8. Murayama T, Iwatsubo R, Akiyama S, Amano A, Morisaki I. Familial hypophosphatemic vitamin D-resistant rickets: dental findings and histologic study of teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2000; 90:310–316.
Article9. Chaussain-Miller C, Sinding C, Septier D, Wolikow M, Goldberg M, Garabedian M. Dentin structure in familial hypophosphatemic rickets: benefits of vitamin D and Dental management in X-linked hypophosphatemia phosphate treatment. Oral Dis. 2007; 13:482–489.
Article10. Zambrano M, Nikitakis NG, Sanchez-Quevedo MC, Sauk JJ, Sedano H, Rivera H. Oral and dental manifestations of vitamin D-dependent rickets type I: report of a pediatric case. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2003; 95:705–709.
Article11. Baroncelli GI, Angiolini M, Ninni E, Galli V, Saggese R, Giuca MR. Prevalence and pathogenesis of dental and periodontal lesions in children with X-linked hypophosphatemic rickets. Eur J Paediatr Dent. 2006; 7:61–66.12. Douyere D, Joseph C, Gaucher C, Chaussain C, Courson F. Familial hypophosphatemic vitamin D-resistant rickets-prevention of spontaneous dental abscesses on primary teeth: a case report. Oral Surg Oral Med Oral Pathol Oral Radiol Endod. 2009; 107:525–530.
Article13. Opsahl Vital S, Gaucher C, Bardet C, Rowe PS, George A, Linglart A, Chaussain C. Tooth dentin defects reflect genetic disorders affecting bone mineralization. Bone. 2012; 50:989–997.
Article14. Holm IA, Nelson AE, Robinson BG, Mason RS, Marsh DJ, Cowell CT, Carpenter TO. Mutational analysis and genotype-phenotype correlation of the PHEX gene in X-linked hypophosphatemic rickets. J Clin Endocrinol Metab. 2001; 86:3889–3899.
Article15. Imel EA, Gray AK, Padgett LR, Econs MJ. Iron and fibroblast growth factor 23 in X-linked hypophosphatemia. Bone. 2014; 60:87–92.
Article16. Resnick D. Implant placement and guided tissue regeneration in a patient with congenital vitamin D-resistant rickets. J Oral Implantol. 1998; 24:214–218.
Article17. Mäkitie O, Doria A, Kooh SW, Cole WG, Daneman A, Sochett E. Early treatment improves growth and biochemical and radiographic outcome in X-linked hypophosphatemic rickets. J Clin Endocrinol Metab. 2003; 88:3591–3597.
Article18. Carpenter TO, Insogna KL, Zhang JH, Ellis B, Nieman S, Simpson C, Olear E, Gundberg CM. Circulating levels of soluble klotho and FGF23 in X-linked hypophosphatemia: circadian variance, effects of treatment, and relationship to parathyroid status. J Clin Endocrinol Metab. 2010; 95:E352–E357.
Article19. Carpenter TO, Imel EA, Holm IA, Jan de Beur SM, Insogna KL. A clinician's guide to X-linked hypophosphatemia. J Bone Miner Res. 2011; 26:1381–1388.
Article20. Tumen EC, Yavuz I, Tumen DS, Atakul F. Dental and histologic findings of X-linked hypophosphataemic vitamin D-resistant rickets: a case report. Int Dent Med Disord. 2008; 1:37–42.21. Seow WK. Diagnosis and management of unusual dental abscesses in children. Aust Dent J. 2003; 48:156–168.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- X-linked hypophosphatemic rickets: from diagnosis to management
- Severe Hypophosphatemia in a Girl with Systemic Lupus Erythematosus
- Carpal Spasm in a Patient with Hypophosphatemia
- Severe hypophosphatemia in hospitalized patients
- Late and Insufficient Phosphorus Supplementation is Associated with Early Severe Hypophosphatemia in Extremely Low Birth Weight Infants with Early Amino Acid Administration
