Ann Dermatol.
2017 Jun;29(3):331-333. 10.5021/ad.2017.29.3.331.
Intense Pulsed Light and Q-Switched 1,064-nm Neodymium-Doped Yttrium Aluminum Garnet Laser Treatment for the Scarring Lesion of Discoid Lupus Erythematosus
- Affiliations
-
- 1Department of Dermatology, Kangnam Sacred Heart Hospital, Hallym University College of Medicine, Seoul, Korea. hyeonekim@gmail.com
- 2Department of Dermatology, Chuncheon Sacred Heart Hospital, Hallym University College of Medicine, Chuncheon, Korea.
- KMID: 2378534
- DOI: http://doi.org/10.5021/ad.2017.29.3.331
Abstract
- Discoid lupus erythematosus (DLE) is a chronic form of cutaneous lupus that can cause permanent scarring. Treatment of DLE includes protection from sunlight and artificial sources of ultraviolet light, as well as systemic and topical medications. The first-line standard therapies are antimalarials and topical steroids. Other systemic therapies include systemic steroid, azathioprine, dapsone, and immunosuppressive agents. Topical tacrolimus and pimecrolimus have also been evaluated. Recent studies reported that several treatments, including pulsed dye laser, COâ‚‚ laser, intense pulsed light (IPL), and 1,064-nm long-pulse neodymium-doped yttrium aluminum (Nd:YAG) have been used for the cosmetic treatment of DLE. Here, we report a case of a DLE scar that was successfully treated with a combination therapy of IPL and Q-switched 1,064-nm Nd:YAG laser.
Keyword
MeSH Terms
Figure
-
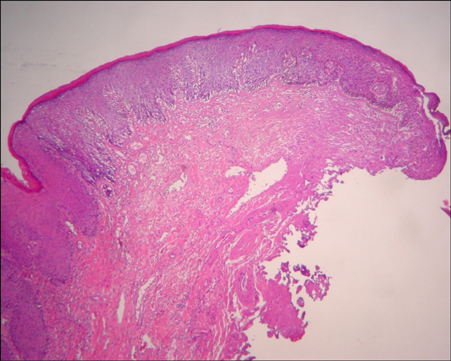
Fig. 1 The epidermis shows vacuolar basal cell degeneration, and the perivascular inflammatory cells infiltrate the upper dermis (H&E, ×40).
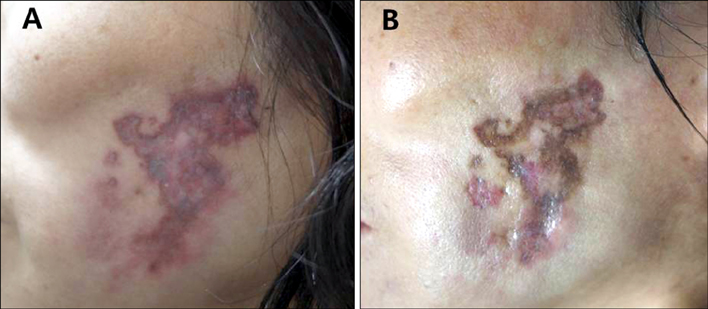
Fig. 2 (A) Before treatment. Sharply demarcated erythematous and hyperpigmented, indurated plaques and atrophic scars on the cheek. (B) After only intense pulsed light treatment. It resolved the erythematous lesions but not the hyperpigmentation.

Fig. 3 After the third session of combined treatment of intense pulsed light and Q-switched 1,064-nm Nd:YAG treatment. The skin lesion showed marked improvement.
Reference
-
1. Walling HW, Sontheimer RD. Cutaneous lupus erythematosus: issues in diagnosis and treatment. Am J Clin Dermatol. 2009; 10:365–381.2. Han YW, Kim HO, Park SH, Park YM. Four cases of facial discoid lupus erythematosus successfully treated with topical pimecrolimus or tacrolimus. Ann Dermatol. 2010; 22:307–311.
Article3. Tzellos TG, Kouvelas D. Topical tacrolimus and pimecrolimus in the treatment of cutaneous lupus erythematosus: an evidence-based evaluation. Eur J Clin Pharmacol. 2008; 64:337–341.
Article4. Ekbäck MP, Troilius A. Laser therapy for refractory discoid lupus erythematosus when everything else has failed. J Cosmet Laser Ther. 2013; 15:260–265.
Article5. Park KY, Lee JW, Li K, Seo SJ, Hong CK. Treatment of refractory discoid lupus erythematosus using 1,064-nm long-pulse neodymium-doped yttrium aluminum garnet laser. Dermatol Surg. 2011; 37:1055–1056.
Article6. Brauer JA, Gordon Spratt EA, Geronemus RG. Laser therapy in the treatment of connective tissue diseases: a review. Dermatol Surg. 2014; 40:1–13.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Perioral Hyperpigmentation Treated with 1,064-nm Q-switched Neodymium:Yttrium-aluminum-garnet Laser Toning
- Acquired Dermal Melanocytosis of the Nose Successfully Treated with Neodymium-doped Yttrium Aluminum Garnet 1064 nm Laser
- Therapeutic effect of long-pulsed 1,064-nm Nd:YAG lasers on venous lakes in Korean patients: a case report
- Partial Unilateral Lentiginosis Successfully Treated with a High-fluence 1,064-nm Q-switched Neodymium:Yttriumaluminum-garnet Laser
- A Split-Face, Single-Blinded, Randomized Controlled Comparison of 532 nm Picosecond Neodymium-Doped Yttrium Aluminum Garnet Laser versus 532 nm Q-Switched Neodymium-Doped Yttrium Aluminum Garnet Laser in the Treatment of Solar Lentigines
