Treatment Options for the Nonunions with Critical Sized Bone Loss
- Affiliations
-
- 1Department of Orthopedic Surgery, Korea University Guro Hospital, Seoul, Korea. jkoh@korea.ac.kr
- KMID: 2376615
- DOI: http://doi.org/10.12671/jkfs.2017.30.2.89
Abstract
- The management of nonunion with severe bone loss is a challenging task to both surgeons and patients. It often requires prolonged and potentially painful treatments. Moreover, it also represents serious socioeconomic issues for patients. Inadequate fracture stability, disrupted biology, such as blood supply and soft tissue, as well as severe bone loss or presence of infection are possible reasons for nonunion. Several different treatment modalities are available, including nail dynamization, plate osteosynthesis, exchange nailing, and adjuvant alternatives, such as electrical or ultrasound stimulation. Autogenous bone graft remains the standard method to reconstruct small defects. Distraction osteogenesis and induced membrane techniques are contemporary strategies of choice for the reconstruction of larger bony defects. Herein, we attempt to describe the key techniques that may be employed in treating nonunion with severe bone loss.
Figure
-

Fig. 1 A 25-year-old male with an open type IIIA tibia shaft fracture. Initial management with Ex-Fix and conversion to lateral locked plating.

Fig. 2 There was a severe gap of 35 mm and no callus formation. No signs of loosening or instability of the construct at postoperative 9 months.

Fig. 3 The fixation structure was stable. Hence, just autogenous bone graft was performed without any additional fixations.

Fig. 4 (A) Postoperative lateral radiography shows the density of the grafted bone at the posterior defect. Insufficient amount of the grafted bone on the posterolateral side (arrow). (B) Lateral radiography taken 6 weeks after the bone graft shows further resorption of grafted bone (arrow).
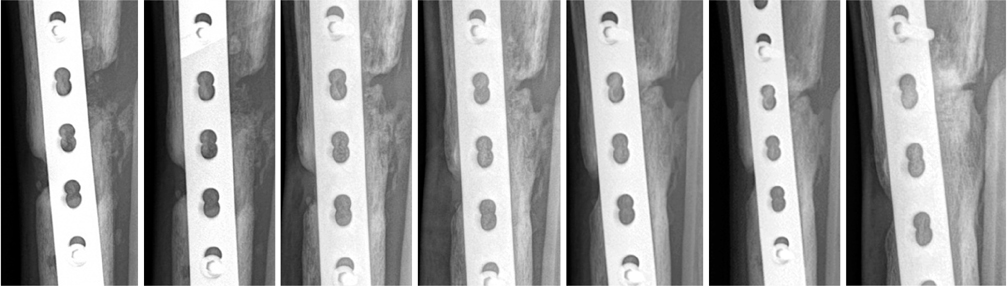
Fig. 5 Serial lateral radiographs show the regeneration of defect site.

Fig. 6 Bone graft should be placed overlapping the bone ends and build up a more fusiform mass.

Fig. 7 (A) Bony consolidation was seen after the X-rays taken at 15th month follow-up. (B) However, there was no bridging of the proximal junction on a computed tomography scan. (C) A dynamization was carried out by remove of screw near the fracture gap. (D) Implant removal was done after union.
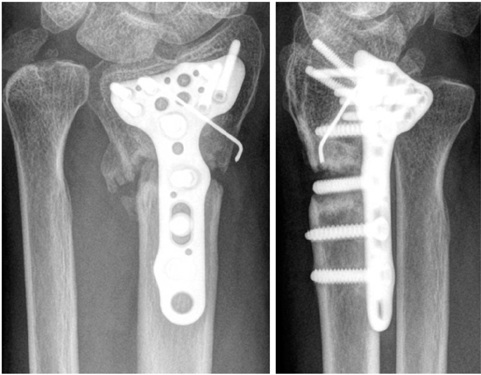
Fig. 8 A 57-year-old male with distal radius fracture. There was 7 mm gap and one screw has inserted through the fracture line.

Fig. 9 Screw was removed from the fracture zone. Autogenous bone graft was placed into the defect.
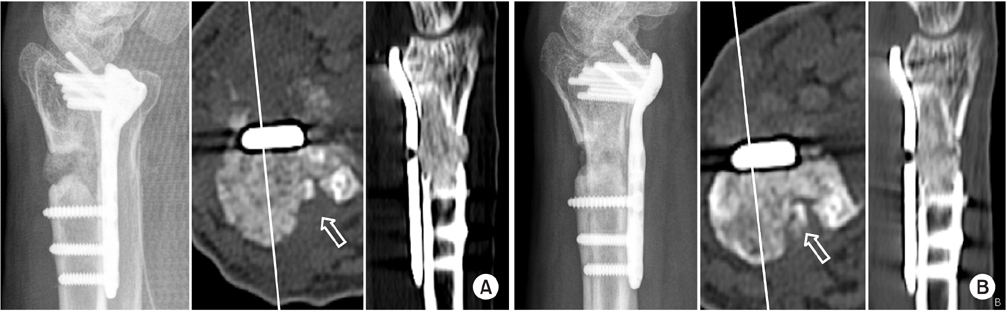
Fig. 10 (A) Postoperative radiograph and computed tomography (CT) scan show an insufficient amount of the grafted bone on the dorsoulnar side (arrow). (B) The volume of the grafted bone was decreased on the radiography and CT scan at 1 month after surgery (arrow).
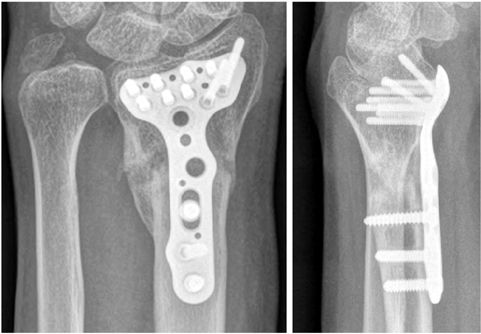
Fig. 11 Well united 6 months after the bone graft.

Fig. 12 A 47-year-old female with femur shaft fracture. She received an open reduction and internal fixation with Intramedullary nailing.
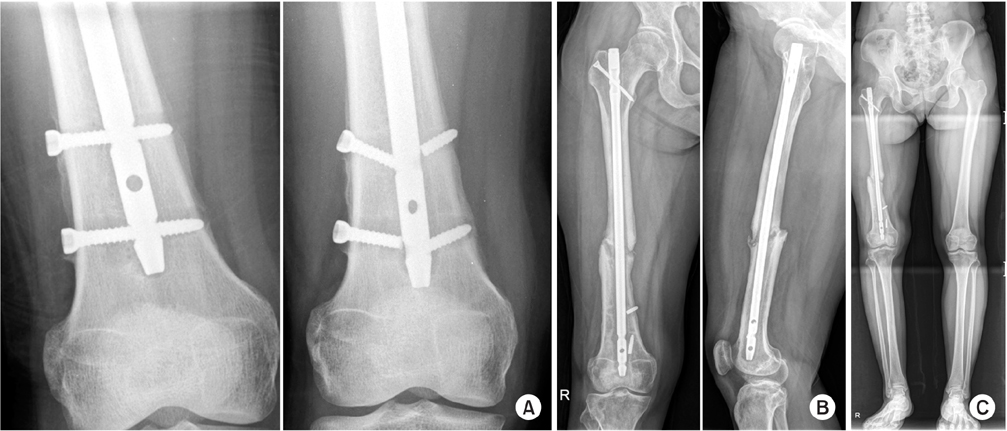
Fig. 13 (A) Loosening of the distal interlocking screws was observed. (B) Screws were broken at 6 months after the surgery. (C) There was 3 cm shortening and callus formation, but no bridging. It was a hypertrophic nonunion.
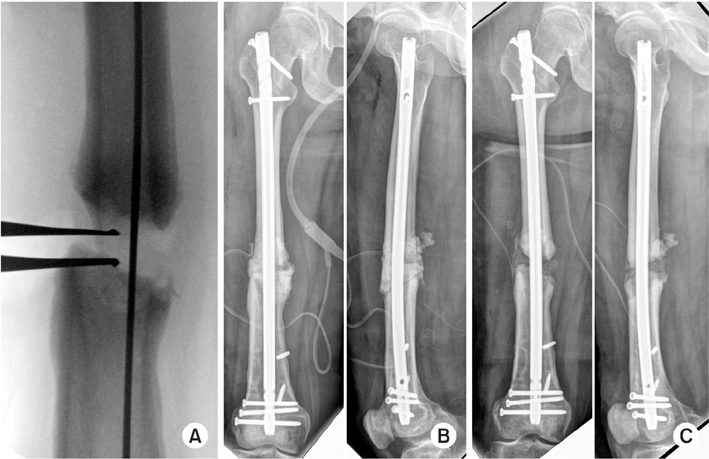
Fig. 14 (A) Acute lengthening was performed using a laminar spreader. (B) Antibiotics (vancomycin+tobramycin) loaded with cement spacer was inserted for bone defect at the nonunion site. (C) Six weeks after the formation of bioactive membrane, autogenous bone graft was performed from the proximal tibia.

Fig. 15 Nine months after autogenous bone graft, defects were well united. Actually, she still has a shortened length of about 7 mm but she was unable to notice any discrepancy in the leg length.

Fig. 16 (A) A 60-year-old male with tibia shaft fracture was treated with Ilizarov and converted plate with autogenous bone graft after 3 months. (B) He was treated with nailing, dynamization, and autogenous bone graft again for nonunion. (C) However, it failed and additional varus collapse had been observed.

Fig. 17 (A) Varus corrections and internal fixations were performed after remove intramedullary nail without sufficient preparation of the nonunion site. The distal screw was broken after 1 year, and the fracture site was still not united. (B) Debrided of sclerotic bone of nonunion site and filled with cement spacer. (C) Autogenous bone graft was carried out and revised the plate construct for add stability.

Fig. 18 (A) A 29-year-old male with bilateral femur shaft fracture and patellar open type I fracture. (B) He received a closed reduction and internal fixation with intramedullary nail.
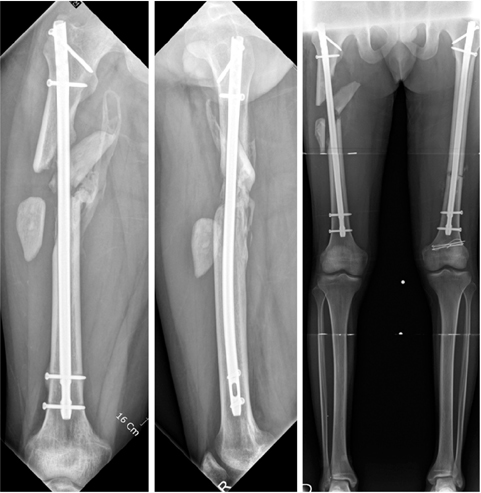
Fig. 19 There were displaced, big wedge fragments. An 85 mm gap was seen.

Fig. 20 Delayed reduction of the vitalized wedge was carried out without soft tissue dissection. Fixation was performed by a mini-plate.

Fig. 21 (A) There was still a gap on the lateral side of the fracture. (B) A dynamization was performed by extraction of the distal interlocking screws. (C) The fracture site was well united.
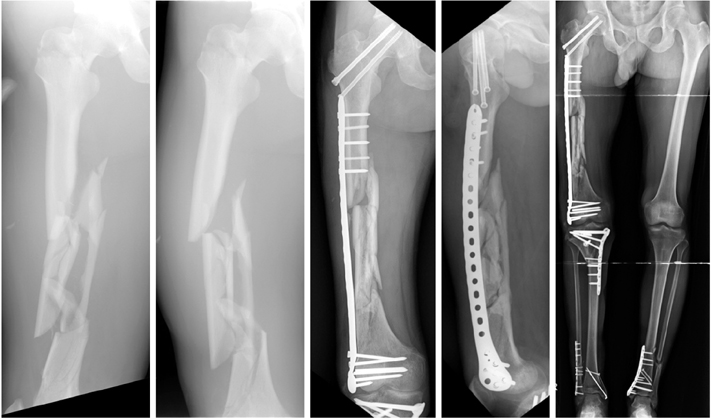
Fig. 22 A 36-year-old male with multiple fractures. There were proximal femur, femur shaft, proximal tibia, and bilateral ankles fractures. Bridging plating was performed with the minimal invasive plate osteosynthesis technique. However, there was no callus.

Fig. 23 (A) Medulostomy was perfromed with a hand reamer, trying to make a pss through the fibricartilagenous tissues and fragments. (B) Reaming was done over the reaming rod. (C) Nail didn't follwo the pass make with flexible reamer because of the rigidity of the nail. (D) Osteotomy was made to the middle wedge fragment to pass the nail along the axis of the bone.

Fig. 24 (A) Postoperative X-rays show that the nail was introduced well along the axis of the femur on the antero-posterior view but the osteotomized middle fragments fell back posteriorly behind the nail on the lateral view. (B) Follow-up X-rays show solid union in good axial and rotational alignment.

Fig. 25 (A) A 28-year-old male presented femur shaft comminuted fracture and tibia shaft fracture. (B) He undertook closed reduction and internal fixation with intramedullary nail.

Fig. 26 (A) Nonunion at the main fracture gap is clearly visible on postoperative 9 months X-rays. (B) Computed tomography images show multiple sites of bone defect in addition to the main nonunion gap. The nature of these multifocal bone defects forced us to choose exchange nailing over augmentation plating and bone graft asbone graft to all these defect sites would be a technically very challenging procedure.

Fig. 27 (A) Simpe exchange nailing was done without bone graft to ignite healing process by reaming and additional stabilty using thicker nail. Radiographs on 1 year after surgery (B), 2 years after surgery (C), and 4 years after surgery (D). Radiographs from the last follow-up showed a solid bony union.
Reference
-
1. Ryaby JT. Clinical effects of electromagnetic and electric fieldson fracture healing. Clin Orthop Relat Res. 1998; 355 Suppl. S205–S215.2. Boyd HB. Symposium: treatment of ununited fractures of the long bones; introduction. J Bone Joint Surg Am. 1965; 47:167–168.3. Connolly JF. Common avoidable problems in nonunions. Clin Orthop Relat Res. 1985; (194):226–235.
Article4. Heckman JD, Sarasohn-Kahn J. The economics of treating tibia fractures. The cost of delayed unions. Bull Hosp Jt Dis. 1997; 56:63–72.5. Bishop JA, Palanca AA, Bellino MJ, Lowenberg DW. Assessment of compromised fracture healing. J Am Acad Orthop Surg. 2012; 20:273–282.
Article6. Services DoHaH. Medicare claims processing manual. Baltimore: Centers for Medicare & Medicaid Services;2010.7. Sanders DW, Bhandari M, Guyatt G, et al. Critical-sized defect in the tibia: is it critical? Results from the SPRINT trial. J Orthop Trauma. 2014; 28:632–635.8. Jones AL, Bucholz RW, Bosse MJ, et al. Recombinant human BMP-2 and allograft compared with autogenous bone graft for reconstruction of diaphyseal tibial fractures with cortical defects. A randomized, controlled trial. J Bone Joint Surg Am. 2006; 88:1431–1441.
Article9. Oh JK, Hwang JH, Lee SJ, Kim JI. Dynamization of locked plating on distal femur fracture. Arch Orthop Trauma Surg. 2011; 131:535–539.
Article10. Dreiseidler T, Kaunisaho V, Neugebauer J, Zöller JE, Rothamel D, Kreppel M. Changes in volume during the four months' remodelling period of iliac crest grafts in reconstruction of the alveolar ridge. Br J Oral Maxillofac Surg. 2016; 54:751–756.
Article11. Sbordone L, Toti P, Menchini-Fabris GB, Sbordone C, Piombino P, Guidetti F. Volume changes of autogenous bone grafts after alveolar ridge augmentation of atrophic maxillae and mandibles. Int J Oral Maxillofac Surg. 2009; 38:1059–1065.
Article12. Macey LR, Kana SM, Jingushi S, Terek RM, Borretos J, Bolander ME. Defects of early fracture-healing in experimental diabetes. J Bone Joint Surg Am. 1989; 71:722–733.
Article13. Oh JK, Bae JH, Oh CW, Biswal S, Hur CR. Treatment of femoral and tibial diaphyseal nonunions using reamed intramedullary nailing without bone graft. Injury. 2008; 39:952–959.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Ilizarov Method for Treatment of Tibia Nonunion Associated with Bone Defects
- The Treatment of Infected Nonunions of Femur using Sequestrectomy and Distraction Osteogenesis
- The Treatment of Infected Nonunions of the Tibia by the Methods of Ilizarov
- Treatment of Femoral Shaft Nonunions with Dynamic Compression using Interlocking-Compression (IC) Nail
- The Operative Treatment of Nonunions of Midshaft Clavicular Fractures: Reconstruction Plate Fixation and Bone Grafting
