Korean J Endocr Surg.
2010 Dec;10(4):213-219. 10.16956/kjes.2010.10.4.213.
Changes of Thyroid Function in Patients Undergoing Partial Thyroidectomy for Benign Thyroid Tumors
- Affiliations
-
- 1Department of Surgery, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. jhkim15@skku.edu
- KMID: 2375471
- DOI: http://doi.org/10.16956/kjes.2010.10.4.213
Abstract
- PURPOSE
Lobectomy or subtotal thyroidectomy in patients with a benign thyroid tumor or goiter can give rise to hypothyroidism due to the reduced volume of the hormone-secreting thyroid gland. This study investigated the incidence of hypothyroidism in such patients and the clinical risk factors.
METHODS
One hundred seven patients who underwent partial thyroidectomy for benign thyroid tumor or goiter from January 2003 to February 2005 in our institution were reviewed retrospectively. Patients who had been preoperatively diagnosed with hyper- or hypothyroidism preoperatively were excluded. Postoperative hypothyroidism was defined as an elevated serum thyroid stimulating hormone (TSH) level >6.5 µIU/L at about 6 months postthyroidectomy.
RESULTS
The mean age of the 107 patients was 42.2 years. Ninety patients (84.1%) were female. Subtotal thyroidectomy was performed in 20 patients, lobectomy in 83 patients and enucleation in four patients. The most common pathologic diagnosis was nodular hyperplasia (86.0%). Postoperative hypothyroidism developed after surgery in 19 (21.8%) patients. Patients were evaluated for age, gender, preoperative TSH level, tumor size, tumor number, extent of the resection, thickness of thyroid isthmus and the presence of pathologic thyroiditis or thyroid autoantibody. Advanced age, elevated preoperative TSH level and extensive resection of the thyroid gland were significantly associated with postoperative hypothyroidism.
CONCLUSION
Since many patients with a benign thyroid nodule can maintain a normal thyroid function even after thyroidectomy, preservation of more thyroid tissue during the operation is desirable, especially in young patients with a low-normal TSH level, unless the possibility of disease recurrence is high.
Keyword
MeSH Terms
Figure
-
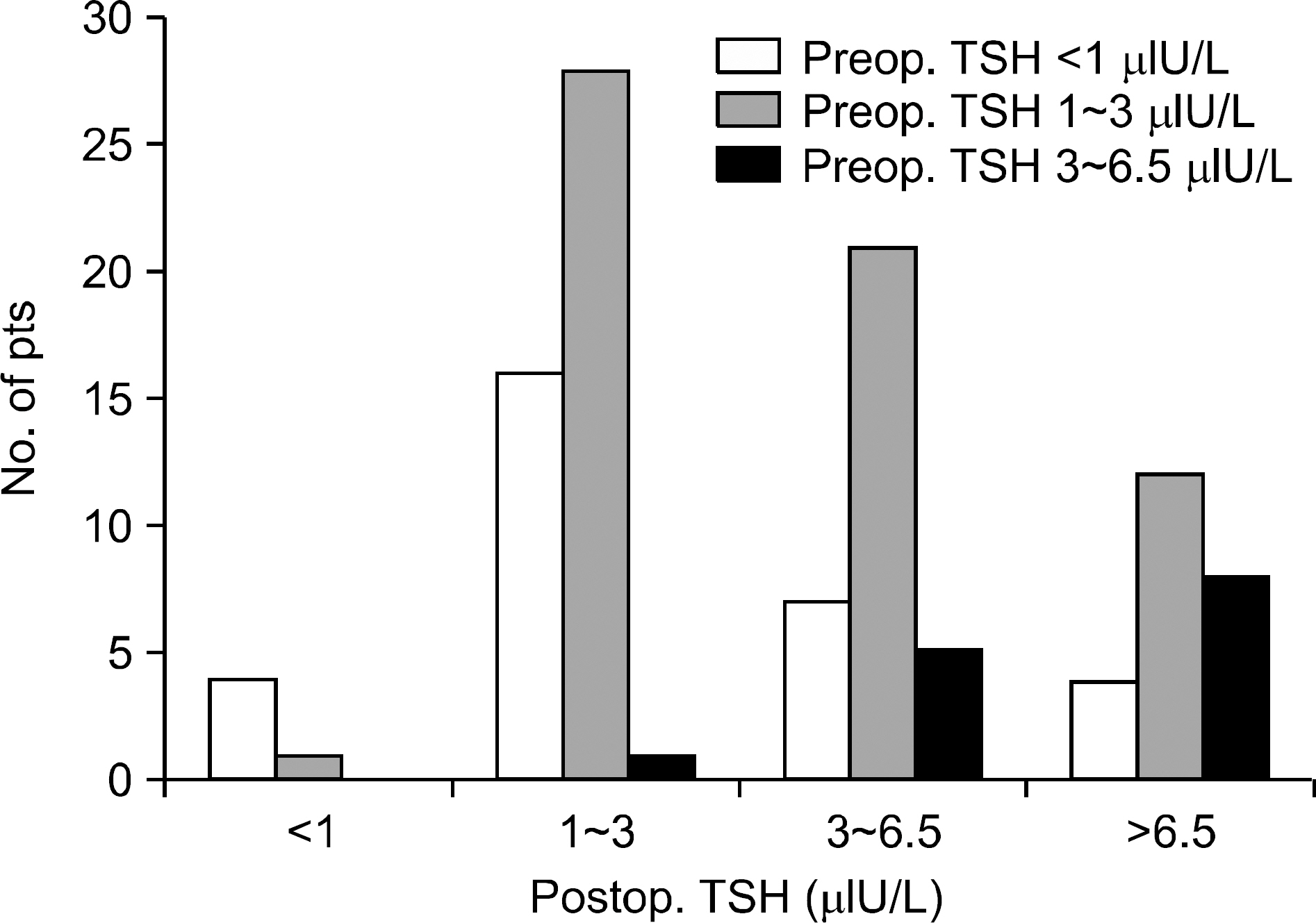
Fig. 1 Changes of serum TSH after thyroidectomy.
Reference
-
1.McGrogan A., Seaman HE., Wright JW., de Vries CS. The incidence of autoimmune thyroid disease: a systematic review of the literature. Clin Endocrinol (Oxf). 2008. 69:687–96.
Article2.Davies L., Welch HG. Increasing incidence of thyroid cancer in the United States, 1973-2002. JAMA. 2006. 295:2164–7.
Article3.Devdhar M., Ousman YH., Burman KD. Hypothyroidism. Endocrinol Metab Clin North Am. 2007. 36:595–615. v.
Article4.Sung TY., Kim YS., Lee SH., Yoon JH., Hong SJ. Surgical treatment of Graves' Disease: comparison between total thyroidectomy and subtotal thyroidectomy. J Korean Surg Soc. 2009. 77:82–7.
Article5.Noh SH., Soh EY., Park CS., Lee KS., Huh KB. Evaluation of thyroid function after bilateral subtotal thyroidectomy for Graves' disease–a long term follow up of 100 patients. Yonsei Med J. 1994. 35:177–83.6.Sawin CT., Geller A., Wolf PA., Belanger AJ., Baker E., Bacharach P, et al. Low serum thyrotropin concentrations as a risk factor for atrial fibrillation in older persons. N Engl J Med. 1994. 331:1249–52.
Article7.Bauer DC., Ettinger B., Nevitt MC., Stone KL. Risk for fracture in women with low serum levels of thyroid-stimulating hormone. Ann Intern Med. 2001. 134:561–8.
Article8.Vaiman M., Nagibin A., Hagag P., Buyankin A., Olevson J., Shlamkovich N. Subtotal and near total versus total thyroidectomy for the management of multinodular goiter. World J Surg. 2008. 32:1546–51.
Article9.McHenry CR., Slusarczyk SJ. Hypothyroidisim following hemithyroidectomy: incidence, risk factors, and management. Surgery. 2000. 128:994–8.
Article10.Miller FR., Paulson D., Prihoda TJ., Otto RA. Risk factors for the development of hypothyroidism after hemithyroidectomy. Arch Otolaryngol Head Neck Surg. 2006. 132:36–8.
Article11.Wormald R., Sheahan P., Rowley S., Rizkalla H., Toner M., Timon C. Hemithyroidectomy for benign thyroid disease: who needs follow-up for hypothyroidism? Clin Otolaryngol. 2008. 33:587–91.
Article12.Koh YW., Lee SW., Choi EC., Lee JD., Mok JO., Kim HK, et al. Prediction of hypothyroidism after hemithyroidectomy: a biochemical and pathological analysis. Eur Arch Otorhino-laryngol. 2008. 265:453–7.
Article13.Su SY., Grodski S., Serpell JW. Hypothyroidism following hemithyroidectomy: a retrospective review. Ann Surg. 2009. 250:991–4.14.Berglund J., Bondesson L., Christensen SB., Larsson AS., Tibblin S. Indications for thyroxine therapy after surgery for nontoxic benign goitre. Acta Chir Scand. 1990. 156:433–8.15.Vaiman M., Nagibin A., Hagag P., Kessler A., Gavriel H. Hypothyroidism following partial thyroidectomy. Otolaryngol Head Neck Surg. 2008. 138:98–100.
Article16.Bakiri F., Hassaim M., Bourouba MS. Subtotal thyroidectomy for benign multinodular goiter: a 6-month postoperative study of the remnant's function and sonographic aspect. World J Surg. 2006. 30:1096–9.
Article17.Ozbas S., Kocak S., Aydintug S., Cakmak A., Demirkiran MA., Wishart GC. Comparison of the complications of subtotal, near total and total thyroidectomy in the surgical management of multinodular goitre. Endocrine Journal. 2005. 52:199–205.
Article18.Rios A., Rodriguez JM., Balsalobre MD., Torregrosa NM., Tebar FJ., Parrilla P. Results of surgery for toxic multinodular goiter. Surg Today. 2005. 35:901–6.
Article19.Bellantone R., Lombardi CP., Boscherini M., Raffaelli M., Tondolo V., Alesina PF, et al. Predictive factors for recurrence after thyroid lobectomy for unilateral non-toxic goiter in an endemic area: results of a multivariate analysis. Surgery. 2004. 136:1247–51.
Article20.Basili G., Biagini C., Manetti A., Martini F., Biliotti G. Risk of recurrence following partial thyroidectomy for benign lesions. Report of 58 patients 15∼25 years after surgery. Minerva Chir. 2003. 58:321–9.21.Olson SE., Starling J., Chen H. Symptomatic benign multinodular goiter: unilateral or bilateral thyroidectomy? Surgery. 2007. 142:458–61. discussion 61-2.
Article22.Phitayakorn R., McHenry CR. Follow-up after surgery for benign nodular thyroid disease: evidence-based approach. World J Surg. 2008. 32:1374–84.
Article23.Hedley AJ., Bewsher PD., Jones SJ., Khir AS., Clements P., Matheson NA, et al. Late onset hypothyroidism after subtotal thyroidectomy for hyperthyroidism: implications for long term follow-up. Br J Surg. 1983. 70:740–3.
Article
