Radiologic Findings and Patient Factors Associated with 30-Day Mortality after Surgical Evacuation of Subdural Hematoma in Patients Less Than 65 Years Old
- Affiliations
-
- 1Department of Neurosurgery, Hanyang University Guri Hospital, Guri, Korea. ryujeil@hanmail.net
- 2Department of Neurosurgery, Hanyang University Medical Center, Seoul, Korea.
- KMID: 2374887
- DOI: http://doi.org/10.3340/jkns.2016.0404.009
Abstract
OBJECTIVE
The purpose of this study is to evaluate the associations between 30-day mortality and various radiological and clinical factors in patients with traumatic acute subdural hematoma (SDH). During the 11-year study period, young patients who underwent surgery for SDH were followed for 30 days. Patients who died due to other medical comorbidities or other organ problems were not included in the study population.
METHODS
From January 1, 2004 to December 31, 2014, 318 consecutive surgically-treated traumatic acute SDH patients were registered for the study. The Kaplan-Meier method was used to analyze 30-day survival rates. We also estimated the hazard ratios of various variables in order to identify the independent predictors of 30-day mortality.
RESULTS
We observed a negative correlation between 30-day mortality and Glasgow coma scale score (per 1-point score increase) (hazard ratio [HR], 0.60; 95% confidence interval [CI], 0.52-0.70; p<0.001). In addition, use of antithrombotics (HR, 2.34; 95% CI, 1.27-4.33; p=0.008), history of diabetes mellitus (HR, 2.28; 95% CI, 1.20-4.32; p=0.015), and accompanying traumatic subarachnoid hemorrhage (hazard ratio, 2.13; 95% CI, 1.27-3.58; p=0.005) were positively associated with 30-day mortality.
CONCLUSION
We found significant associations between short-term mortality after surgery for traumatic acute SDH and lower Glasgow Coma Scale scores, use of antithrombotics, history of diabetes mellitus, and accompanying traumatic subarachnoid hemorrhage at admission. We expect these findings to be helpful for selecting patients for surgical treatment of traumatic acute SDH, and for making accurate prognoses.
MeSH Terms
Figure
-
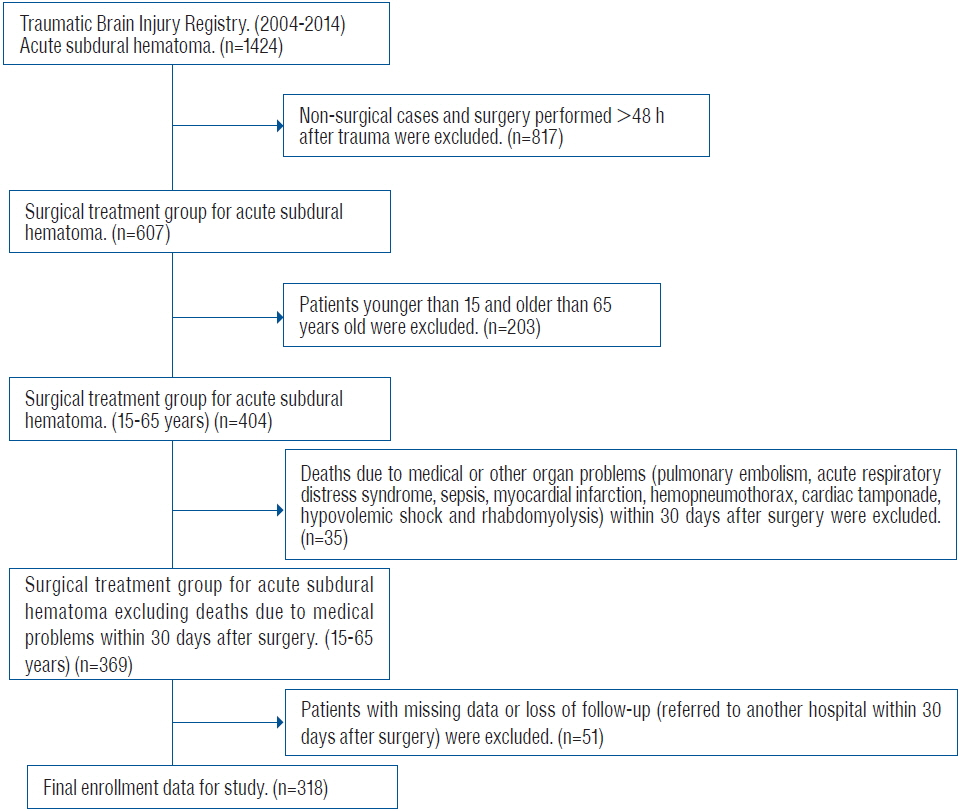
Fig. 1 Flow chart of the process for selecting eligible patients from our hospital’s Traumatic Brain Injury registry during the period from January 1, 2004 to December 31, 2014.
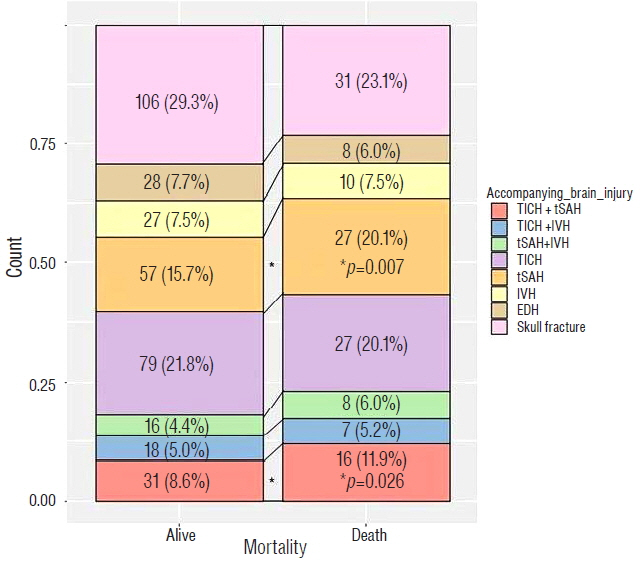
Fig. 2 Dichotomized analysis of the distribution of initial accompanying brain injuries in patients who survived or died within 30 days of surgery for acute subdural hematoma. TICH: traumatic intracerebral hematoma, tSAH: traumatic subarachnoid hemorrhage, IVH: intraventricular blood, EDH: epidural hematoma. * p<0.05.
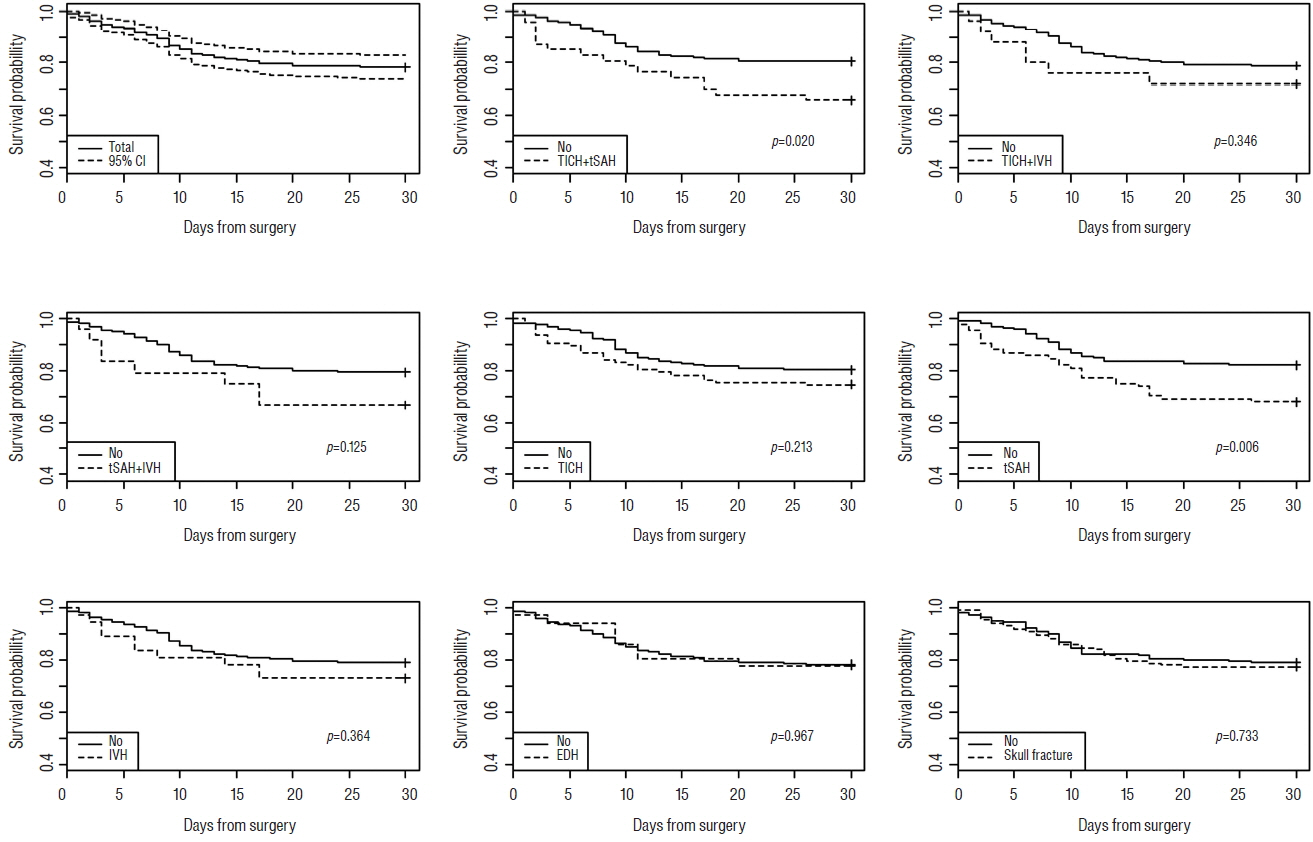
Fig. 3 Kaplan–Meier curve with log-rank test showing survival probability within 30 days of surgery, based on initial accompanying brain injury. CI: conÿdence interval, TICH: traumatic intracerebral hematoma, tSAH: traumatic subarachnoid hemorrhage, IVH: intraventricular blood, EDH: epidural hematoma.
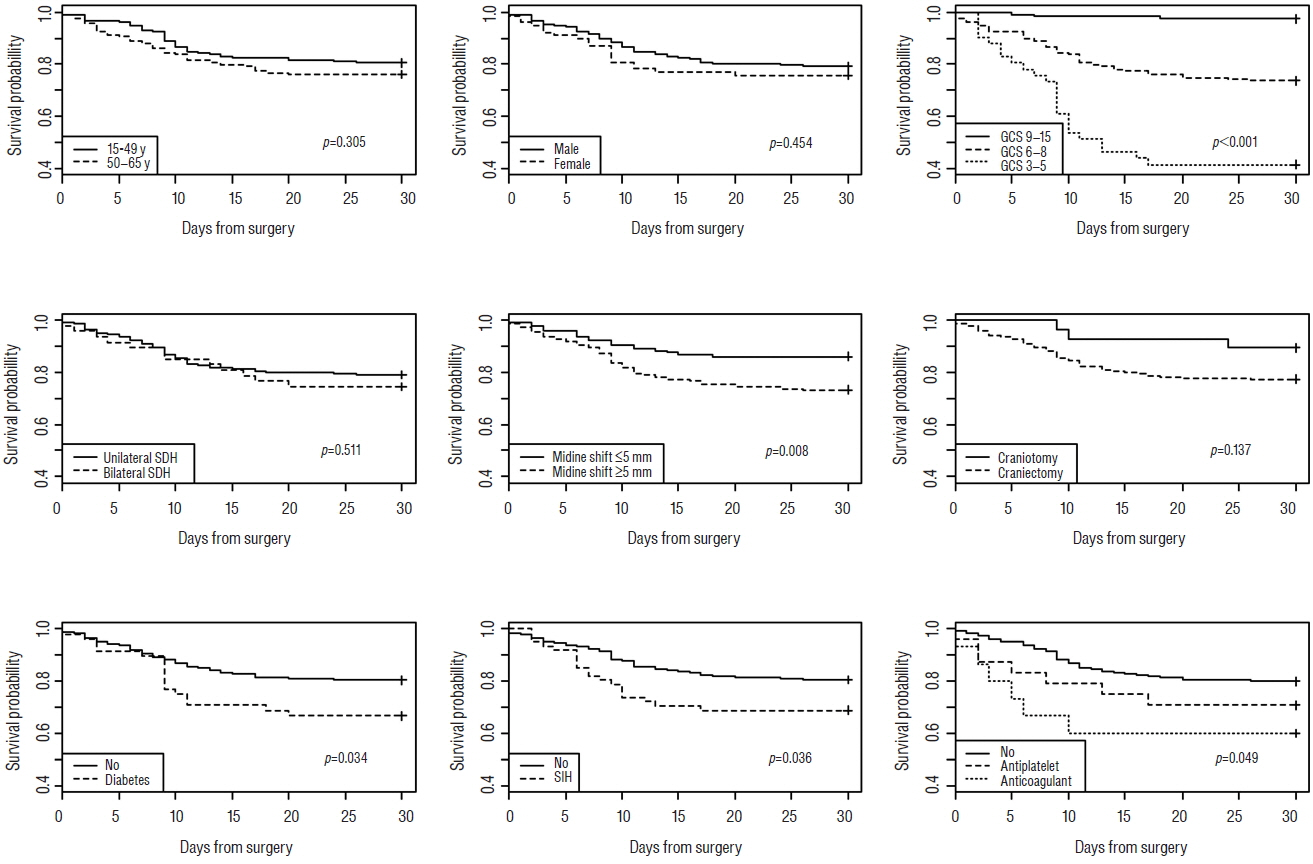
Fig. 4 Kaplan–Meier curve with log-rank test showing survival probability within 30 days of surgery based on clinical and radiologic factors. GCS: Glasgow coma scale, SDH: subdural hematoma, SIH: stress-induced hyperglycemia.
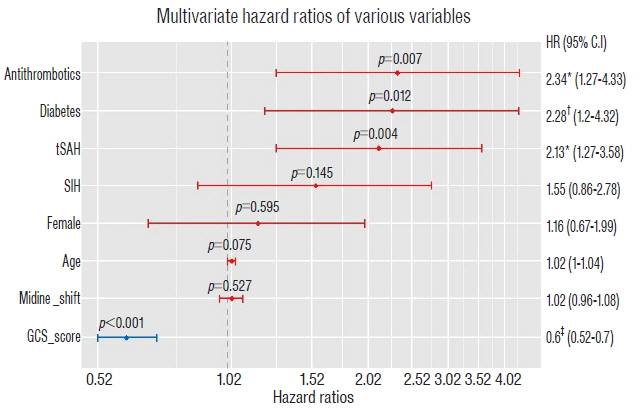
Fig. 5 Multivariate hazard ratios of clinical and radiologic factors associated with 30-day mortality after surgery. HR: hazard ratio, CI: confidence interval, tSAH: traumatic subarachnoid hemorrhage, SIH: stress-induced hyperglycemia, GCS: Glasgow coma scale. *p<0.01, †p<0.05, ‡p<0.001.
Reference
-
References
1. Aarabi B, Hesdorffer DC, Ahn ES, Aresco C, Scalea TM, Eisenberg HM. Outcome following decompressive craniectomy for malignant swelling due to severe head injury. J Neurosurg. 104:469–479. 2006.
Article2. Aminmansour B, Ghorbani A, Sharifi D, Shemshaki H, Ahmadi A. Cerebral vasospasm following traumatic subarachnoid hemorrhage. J Res Med Sci. 14:343–348. 2009.3. Beynon C, Potzy A, Sakowitz OW, Unterberg AW. Rivaroxaban and intracranial haemorrhage after mild traumatic brain injury: A dangerous combination? Clin Neurol Neurosurg. 136:73–78. 2015.
Article4. Bosarge PL, Shoultz TH, Griffin RL, Kerby JD. Stress-induced hyperglycemia is associated with higher mortality in severe traumatic brain injury. J Trauma Acute Care Surg. 79:289–294. 2015.
Article5. Cepeda S, Gómez PA, Castaño-Leon AM, Martínez-Pérez R, Munarriz PM, Lagares A. Traumatic intracerebral hemorrhage: risk factors associated with progression. J Neurotrauma. 32:1246–1253. 2015.
Article6. Collins CE, Witkowski ER, Flahive JM, Anderson FA Jr, Santry HP. Effect of preinjury warfarin use on outcomes after head trauma in Medicare beneficiaries. Am J Surg. 208:544–549.e1. 2014.
Article7. Devereaux PJ, Mrkobrada M, Sessler DI, Leslie K, Alonso-Coello P, Kurz A, et al. Aspirin in patients undergoing noncardiac surgery. N Engl J Med. 370:1494–1503. 2014.8. Fisher CM, Kistler JP, Davis JM. Relation of cerebral vasospasm to subarachnoid hemorrhage visualized by computerized tomographic scanning. Neurosurgery. 6:1–9. 1980.
Article9. Franko J, Kish KJ, O’Connell BG, Subramanian S, Yuschak JV. Advanced age and preinjury warfarin anticoagulation increase the risk of mortality after head trauma. J Trauma. 61:107–110. 2006.
Article10. Gómez PA, de-la-Cruz J, Lora D, Jiménez-Roldán L, Rodríguez-Boto G, Sarabia R, et al. Validation of a prognostic score for early mortality in severe head injury cases. J Neurosurg. 121:1314–1322. 2014.
Article11. Grandhi R, Harrison G, Voronovich Z, Bauer J, Chen SH, Nicholas D, et al. Preinjury warfarin, but not antiplatelet medications, increases mortality in elderly traumatic brain injury patients. J Trauma Acute Care Surg. 78:614–621. 2015.
Article12. Griesdale DE, Tremblay MH, McEwen J, Chittock DR. Glucose control and mortality in patients with severe traumatic brain injury. Neurocrit Care. 11:311–316. 2009.
Article13. Howard MA 3rd, Gross AS, Dacey RG Jr, Winn HR. Acute subdural hematomas: an age-dependent clinical entity. J Neurosurg. 71:858–863. 1989.
Article14. Huang YH, Lee TC, Lee TH, Liao CC, Sheehan J, Kwan AL. Thirty-day mortality in traumatically brain-injured patients undergoing decompressive craniectomy. J Neurosurg. 118:1329–1335. 2013.
Article15. Jeremitsky E, Omert LA, Dunham CM, Wilberger J, Rodriguez A. The impact of hyperglycemia on patients with severe brain injury. J Trauma. 58:47–50. 2005.
Article16. Karibe H, Hayashi T, Hirano T, Kameyama M, Nakagawa A, Tominaga T. Surgical management of traumatic acute subdural hematoma in adults: a review. Neurol Med Chir (Tokyo). 54:887–894. 2014.
Article17. Kenney K, Amyot F, Haber M, Pronger A, Bogoslovsky T, Moore C, et al. Cerebral vascular injury in traumatic brain injury. Exp Neurol 275 Pt. 3:353–366. 2016.
Article18. Khoury JC, Kleindorfer D, Alwell K, Moomaw CJ, Woo D, Adeoye O, et al. Diabetes mellitus: a risk factor for ischemic stroke in a large biracial population. Stroke J Cereb Circ. 44:1500–1504. 2013.19. Kothari RU, Brott T, Broderick JP, Barsan WG, Sauerbeck LR, Zuccarello M, et al. The ABCs of measuring intracerebral hemorrhage volumes. Stroke. 27:1304–1305. 1996.
Article20. Ley EJ, Srour MK, Clond MA, Barnajian M, Tillou A, Mirocha J, et al. Diabetic patients with traumatic brain injury: insulin deficiency is associated with increased mortality. J Trauma. 70:1141–1144. 2011.
Article21. Liu S, Wan X, Wang S, Huang L, Zhu M, Zhang S, et al. Posttraumatic cerebral infarction in severe traumatic brain injury: characteristics, risk factors and potential mechanisms. Acta Neurochir (Wien). 157:1697–1704. 2015.
Article22. Liu-DeRyke X, Collingridge DS, Orme J, Roller D, Zurasky J, Rhoney DH. Clinical impact of early hyperglycemia during acute phase of traumatic brain injury. Neurocrit Care. 11:151–157. 2009.
Article23. Logistic Regression Using SAS®: Theory and Application, Second Edition. Available: https://www.sas.com/store/books/categories/usage-and-reference/logistic-regression-using-sas-theory-and-application-second-edition/prodBK_61340_en.html. Accessed 14 October 2015.24. Lukasiewicz AM, Grant RA, Basques BA, Webb ML, Samuel AM, Grauer JN. Patient factors associated with 30-day morbidity, mortality, and length of stay after surgery for subdural hematoma: a study of the American College of Surgeons National Surgical Quality Improvement Program. J Neurosurg. 124:1–7. 2015.
Article25. Lustenberger T, Talving P, Lam L, Inaba K, Bass M, Plurad D, et al. Effect of diabetes mellitus on outcome in patients with traumatic brain injury: a national trauma databank analysis. Brain Inj. 27:281–285. 2013.
Article26. MRC CRASH Trial Collaborators. Perel P, Arango M, Clayton T, Edwards P, Komolafe E, et al. Predicting outcome after traumatic brain injury: practical prognostic models based on large cohort of international patients. BMJ. 336:425–429. 2008.
Article27. Murray GD, Butcher I, McHugh GS, Lu J, Mushkudiani NA, Maas AI, et al. Multivariable prognostic analysis in traumatic brain injury: results from the IMPACT study. J Neurotrauma. 24:329–337. 2007.
Article28. Parchani A, El-Menyar A, Al-Thani H, El-Faramawy A, Zarour A, Asim M, et al. Traumatic subarachnoid hemorrhage due to motor vehicle crash versus fall from height: a 4-year epidemiologic study. World Neurosurg. 82:e639–e644. 2014.
Article29. Rovlias A, Kotsou S. The influence of hyperglycemia on neurological outcome in patients with severe head injury. Neurosurgery. 46:335–342. discussion 342–343. 2000.
Article30. Wojcik R, Cipolle MD, Seislove E, Wasser TE, Pasquale MD. Preinjury warfarin does not impact outcome in trauma patients. J Trauma. 51:1147–1151. discussion 1151–1152. 2001.
Article31. Wong GK, Yeung JH, Graham CA, Zhu XL, Rainer TH, Poon WS. Neurological outcome in patients with traumatic brain injury and its relationship with computed tomography patterns of traumatic subarachnoid hemorrhage. J Neurosurg. 114:1510–1515. 2011.
Article32. Zubkov AY, Lewis AI, Raila FA, Zhang J, Parent AD. Risk factors for the development of post-traumatic cerebral vasospasm. Surg Neurol. 53:126–130. 2000.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Intraoperative Development of Contralateral Subdural Hematoma during Evacuation of Acute Subdural Hematoma: Case Report
- Prognostic Factors of Chronic Subdural Hematoma
- Bilateral Acute Subdural Hematoma Following Evacuation of Chronic Subdural Hematoma
- "Contralateral" Acute Subdural and Intracerebral Hemorrhage Occurring Simultaneously after Evacuation of Huge Chronic Subdural Hematoma
- Spontaneously Rapid Resolution of Acute Subdural Hemorrhage with Severe Midline Shift
