Polyetheretherketone Cage with Demineralized Bone Matrix Can Replace Iliac Crest Autografts for Anterior Cervical Discectomy and Fusion in Subaxial Cervical Spine Injuries
- Affiliations
-
- 1Department of Neurosurgery, Chonnam National University Medical School & Research Institute of Medical Sciences, Gwangju, Korea. genius60@hanmail.net
- 2Department of Neurosurgery, Happy-view Samsung Hospital, Gwangju, Korea.
- KMID: 2374883
- DOI: http://doi.org/10.3340/jkns.2015.0203.014
Abstract
OBJECTIVE
This study aimed to compare the clinical and radiologic outcomes of patients with subaxial cervical injury who underwent anterior cervical discectomy and fusion (ACDF) with autologous iliac bone graft or polyetheretherketone (PEEK) cages using demineralized bone matrix (DBM).
METHODS
From January 2005 to December 2010, 70 patients who underwent one-level ACDF with plate fixation for post-traumatic subaxial cervical spinal injury in a single institution were retrospectively investigated. Autologous iliac crest grafts were used in 33 patients (Group I), whereas 37 patients underwent ACDF using a PEEK cage filled with DBM (Group II). Plain radiographs were used to assess bone fusion, interbody height (IBH), segmental angle (SA), overall cervical sagittal alignment (CSA, C2-7 angle), and development of adjacent segmental degeneration (ASD). Clinical outcome was assessed using a visual analog scale (VAS) for pain and Frankel grade.
RESULTS
The mean follow-up duration for patients in Group I and Group II was 28.9 and 25.4 months, respectively. All patients from both groups achieved solid fusion during the follow-up period. The IBH and SA of the fused segment and CSA in Group II were better maintained during the follow-up period. Nine patients in Group I and two patients in Group II developed radiologic ASD. There were no statistically significant differences in the VAS score and Frankel grade between the groups.
CONCLUSION
This study showed that PEEK cage filled with DBM, and plate fixation is at least as safe and effective as ACDF using autograft, with good maintenance of cervical alignment. With advantages such as no donor site morbidity and no graft-related complications, PEEK cage filled with DBM, and plate fixation provide a promising surgical option for treating traumatic subaxial cervical spine injuries.
Keyword
MeSH Terms
Figure
-
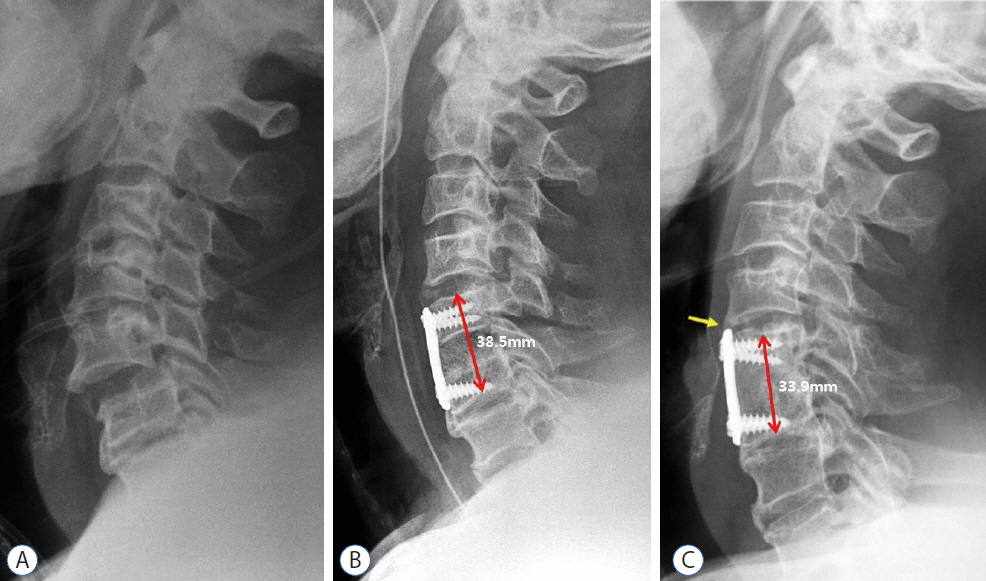
Fig. 1 Imaging studies of a 54-year-old man who underwent a C5–6 anterior cervical fusion using autologous iliac bone graft after subaxial injury. A: Simple cervical lateral radiograph shows C5–6 subluxation and disc space widening with spinous process fracture. B: Postoperative radiograph shows satisfactory reduction of the injured segment after C5–6 fusion with anterior plating. C: Last follow-up radiograph at 24 months after surgery shows satisfactory fusion at the C5–6 level; however, some degrees of subsidence and development of adjacent segment degeneration (yellow arrow) were observed with impingement of the plate to C4–5 disc level.

Fig. 2 Imaging studies of a 47-year-old man who underwent C6–7 fusion using a synthetic cage filled with demineralized bone matrix and local osteophytes. A: Simple cervical lateral radiograph shows C6–7 subluxation and disc space widening. B: Postoperative radiograph shows satisfactory reduction of the injured segment after C6–7 fusion. C: Last follow-up radiograph at 24 months after surgery shows satisfactory fusion at the C6–7 level, without the development of subsidence and junctional problems. D: Computed tomography image shows successful filling of bony tissue within the synthetic cage.
Cited by 3 articles
-
Outcomes of Anterior Cervical Fusion Using Polyetheretherketone Cage with Demineralized Bone Matrix and Plate for Management of Subaxial Cervical Spine Injuries
Moon-Soo Han, Gwang-Jun Lee, Ju-Hwi Kim, Seul-Kee Lee, Bong Ju Moon, Jung-Kil Lee
Korean J Neurotrauma. 2018;14(2):123-128. doi: 10.13004/kjnt.2018.14.2.123.Clinical Efficacy of Cages in Anterior Cervical Fusion for Degenerative Cervical Disease
Moon Soo Park, Woo-Kie Min, Sang-Bong Ko, Young-Yul Kim, Byung-Wan Choi, Jong Hyun Ko
J Korean Soc Spine Surg. 2019;26(4):172-177. doi: 10.4184/jkss.2019.26.4.172.Risk Factors for Prevertebral Soft Tissue Swelling Following Single-Level Anterior Cervical Spine Surgery
Junsang Park, Sang Mook Kang, Yu Deok Won, Myung-Hoon Han, Jin Hwan Cheong, Byeong-Jin Ha, Je Il Ryu
J Korean Neurosurg Soc. 2023;66(6):716-725. doi: 10.3340/jkns.2023.0123.
Reference
-
References
1. Aebi M. Surgical treatment of upper, middle and lower cervical injuries and non-unions by anterior procedures. Eur Spine J. 19(Suppl 1):S33–S39. 2009.
Article2. Bishop RC, Moore KA, Hadley MN. Anterior cervical interbody fusion using autogeneic and allogeneic bone graft substrate: a prospective comparative analysis. J Neurosurg. 85:206–210. 1996.
Article3. Bohlman HH. Acute fractures and dislocations of the cervical spine. An analysis of three hundred hospitalized patients and review of the literature. J Bone Joint Surg Am. 61:1119–1142. 1979.
Article4. Bracken MB, Shepard MJ, Collins WF, Holford TR, Young W, Baskin DS, et al. A randomized, controlled trial of methylprednisolone or naloxone in the treatment of acute spinal-cord injury. Results of the second national acute spinal cord injury study. N Engl J Med. 322:1405–1411. 1990.
Article5. Cauthen JC, Kinard RE, Vogler JB, Jackson DE, DePaz OB, Hunter OL, et al. Outcome analysis of noninstrumented anterior cervical discectomy and interbody fusion in 348 patients. Spine (Phila Pa 1976). 23:188–192. 1998.
Article6. Cho DY, Liau WR, Lee WY, Liu JT, Chiu CL, Sheu PC. Preliminary experience using a polyetheretherketone (PEEK) cage in the treatment of cervical disc disease. Neurosurgery. 51:1343–1349. discussion 1349–1350. 2002.
Article7. Du W, Wang C, Tan J, Shen B, Ni S, Zheng Y. Management of subaxial cervical facet dislocation through anterior approach monitored by spinal cord evoked potential. Spine (Phila Pa 1976). 39:48–52. 2014.
Article8. Fazl M, Pirouzmand F. Intraoperative reduction of locked facets in the cervical spine by use of a modified interlaminar spreader: technical note. Neurosurgery. 48:444–445. discussion 445–446. 2001.
Article9. Feng G, Hong Y, Li L, Liu H, Pei F, Song Y, et al. Anterior decompression and nonstructural bone grafting and posterior fixation for cervical facet dislocation with traumatic disc herniation. Spine (Phila Pa 1976). 37:2082–2088. 2012.
Article10. Frankel HL, Hancock DO, Hyslop G, Melzak J, Michaelis LS, Ungar GH, et al. The value of postural reduction in the initial management of closed injuries of the spine with paraplegia and tetraplegia. I. Paraplegia. 7:179–192. 1969.
Article11. Garvey TA, Eismont FJ, Roberti LJ. Anterior decompression, structural bone grafting, and Caspar plate stabilization for unstable cervical spine fractures and/or dislocations. Spine (Phila Pa 1976). 17:S431–S435. 1992.
Article12. Hadley MN, Fitzpatrick BC, Sonntag VK, Browner CM. Facet fracture-dislocation injuries of the cervical spine. Neurosurgery. 30:661–666. 1992.
Article13. Hilibrand AS, Carlson GD, Palumbo MA, Jones PK, Bohlman HH. Radiculopathy and myelopathy at segments adjacent to the site of a previous anterior cervical arthrodesis. J Bone Joint Surg Am. 81:519–528. 1999.
Article14. Kim KHCD, Sung JK. The management of bilateral interfacetal dislocation with anterior fixation in cervical spine: comparision with combined antero-posterior fixation. J Korean Neurosurg Soc. 42:305–310. 2007.
Article15. Kulkarni AG, Hee HT, Wong HK. Solis cage (PEEK) for anterior cervical fusion: preliminary radiological results with emphasis on fusion and subsidence. Spine J. 7:205–209. 2007.
Article16. Ning X, Wen Y, Xiao-Jian Y, Bin N, De-Yu C, Jian-Ru X, et al. Anterior cervical locking plate-related complications; prevention and treatment recommendations. Int Orthop. 32:649–655. 2008.
Article17. Oh HS, Shim CS, Kim JS, Lee SH. Clinical and radiological comparison of femur and fibular allografts for the treatment of cervical degenerative disc diseases. J Korean Neurosurg Soc. 92:18–23. 2013.
Article18. Park MS, Kelly MP, Lee DH, Min WK, Rahman RK, Riew KD. Sagittal alignment as a predictor of clinical adjacent segment pathology requiring surgery after anterior cervical arthrodesis. Spine J. 14:1228–1234. 2013.
Article19. Paxinos O, Ghanayem AJ, Zindrick MR, Voronov LI, Havey RM, Carandang G, et al. Anterior cervical discectomy and fusion with a locked plate and wedged graft effectively stabilizes flexion-distraction stage-3 injury in the lower cervical spine: a biomechanical study. Spine (Phila Pa 1976). 34:E9–E15. 2009.20. Rawlinson JN. Morbidity after anterior cervical decompression and fusion. The influence of the donor site on recovery, and the results of a trial of surgibone compared to autologous bone. Acta Neurochir (Wien). 131:106–118. 1994.
Article21. Reindl R, Ouellet J, Harvey EJ, Berry G, Arlet V. Anterior reduction for cervical spine dislocation. Spine (Phila Pa 1976). 31:648–652. 2006.
Article22. Riew KD, Rhee JM. The use of titanium mesh cages in the cervical spine. Clin Orthop Relat Res. 47–54. 2002.
Article23. Rizzolo SJ, Piazza MR, Cotler JM, Balderston RA, Schaefer D, Flanders A. Intervertebral disc injury complicating cervical spine trauma. Spine (Phila Pa 1976). 16:S187–S189. 1991.
Article24. Robertson PA, Ryan MD. Neurological deterioration after reduction of cervical subluxation. Mechanical compression by disc tissue. J Bone Joint Surg Br. 74:224–227. 1992.
Article25. Shapiro S, Snyder W, Kaufman K, Abel T. Outcome of 51 cases of unilateral locked cervical facets: interspinous braided cable for lateral mass plate fusion compared with interspinous wire and facet wiring with iliac crest. J Neurosurg. 91:19–24. 1999.
Article26. Song KJ, Choi BW, Kim GH, Song JH. Usefulness of polyetheretherketone (PEEK) cage with plate augmentation for anterior arthrodesis in traumatic cervical spine injury. Spine J. 10:50–57. 2010.
Article27. Thome C, Krauss JK, Zevgaridis D. A prospective clinical comparison of rectangular titanium cages and iliac crest autografts in anterior cervical discectomy and fusion. Neurosurg Rev. 27:34–41. 2004.
Article28. Vavruch L, Hedlund R, Javid D, Leszniewski W, Shalabi A. A prospective randomized comparison between the cloward procedure and a carbon fiber cage in the cervical spine: a clinical and radiologic study. Spine. 27:1694–1701. 2002.
Article29. Vital JM, Gille O, Senegas J, Pointillart V. Reduction technique for uni- and biarticular dislocations of the lower cervical spine. Spine. 23:949–954. discussion 955. 1998.
Article30. Yamagata T, Takami T, Uda T, Ikeda H, Nagata T, Sakamoto S, et al. Outcomes of contemporary use of rectangular titanium stand-alone cages in anterior cervical discectomy and fusion: cage subsidence and cervical alignment. J Clin Neurosci. 19:1673–1678. 2012.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Outcomes of Anterior Cervical Fusion Using Polyetheretherketone Cage with Demineralized Bone Matrix and Plate for Management of Subaxial Cervical Spine Injuries
- Anterior Cervical Discectomy and Fusion Using a Stand-Alone Polyetheretherketone Cage Packed with Local Autobone : Assessment of Bone Fusion and Subsidence
- Efficiency of Anterior Interbody Fusion using Cage Packed with DBM in the Distractive Flexion Injury of Cervical Spine: Demineralized Bone Matrix vs Autoiliac Cancellous Bone
- A Prospective Randomized Clinical Trial Comparing Bone Union Rate Following Anterior Cervical Discectomy and Fusion Using a Polyetheretherketone Cage: Hydroxyapatite/B-Tricalcium Phosphate Mixture versus Hydroxyapatite/Demineralized Bone Matrix Mixture
- Comparative Study of Clinical Outcomes of Anterior Cervical Discectomy and Fusion Using Autobone Graft or Cage with Bone Substitute
