Living Donor Liver Transplantation for Advanced Hepatocellular Carcinoma with Portal Vein Tumor Thrombosis after Concurrent Chemoradiation Therapy
- Affiliations
-
- 1Department of Surgery, Yonsei University College of Medicine, Seoul, Korea. soonkim@yuhs.ac
- 2Liver Cancer Special Clinic, Yonsei University College of Medicine, Seoul, Korea. gihankhys@yuhs.ac
- 3Research Institute for Transplantation, Yonsei University College of Medicine, Seoul, Korea.
- 4Department of Pathology, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Radiological Oncology, Yonsei University College of Medicine, Seoul, Korea.
- 6Department of Internal Medicine, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2374176
- DOI: http://doi.org/10.3349/ymj.2016.57.5.1276
Abstract
- Locally advanced hepatocellular carcinoma (HCC) with portal vein thrombosis carries a 1-year survival rate <10%. Localized concurrent chemoradiotherapy (CCRT), followed by hepatic arterial infusion chemotherapy (HAIC), was recently introduced in this setting. Here, we report our early experience with living donor liver transplantation (LDLT) in such patients after successful down-staging of HCC through CCRT and HAIC. Between December 2011 and September 2012, eight patients with locally advanced HCC at initial diagnosis were given CCRT, followed by HAIC, and underwent LDLT at the Severance Hospital, Seoul, Korea. CCRT [45 Gy over 5 weeks with 5-fluorouracil (5-FU) as HAIC] was followed by HAIC (5-FU/cisplatin combination every 4 weeks for 3-12 months), adjusted for tumor response. Down-staging succeeded in all eight patients, leaving no viable tumor thrombi in major vessels, although three patients first underwent hepatic resections. Due to deteriorating liver function, transplantation was the sole therapeutic option and offered a chance for cure. The 1-year disease-free survival rate was 87.5%. There were three instances of post-transplantation tumor recurrence during follow-up monitoring (median, 17 months; range, 10-22 months), but no deaths occurred. Median survival time from initial diagnosis was 33 months. Four postoperative complications recorded in three patients (anastomotic strictures: portal vein, 2; bile duct, 2) were resolved through radiologic interventions. Using an intensive tumor down-staging protocol of CCRT followed by HAIC, LDLT may be a therapeutic option for selected patients with locally advanced HCC and portal vein tumor thrombosis.
Keyword
MeSH Terms
-
Adult
Carcinoma, Hepatocellular/complications/drug therapy/surgery/*therapy
*Chemoradiotherapy
Cisplatin/therapeutic use
Disease-Free Survival
Female
Fluorouracil/therapeutic use
Humans
Liver Neoplasms/complications/drug therapy/surgery/*therapy
*Liver Transplantation
*Living Donors
Male
Middle Aged
Neoplasm Recurrence, Local
*Portal Vein
Venous Thrombosis/*complications
Cisplatin
Fluorouracil
Figure
-

Fig. 1 Events leading to liver transplantation: overall, eight patients underwent living donor liver transplantation (LDLT) after concurrent chemoradiotherapy, followed by hepatic arterial infusion chemotherapy. Advanced status of tumor (with portal vein tumor thrombosis) was initially down-staged via pre-transplant regimen. In five patients, transplantations constituted rescue therapy for hepatic decompensation. *The patient underwent LDLT after down-staging for recurred HCC without decompensated liver failure. CCRT, concurrent chemoradiotherapy; HAIC, hepatic arterial infusion chemotherapy; HCC, hepatocellular carcinoma; PR, partial response.

Fig. 2 Radiologic tumor response (to concurrent chemoradiotherapy, followed by hepatic arterial infusion chemotherapy): computed tomography demonstrates bulky 12 cm hepatocellular carcinoma of right lobe (A), decreasing to 6 cm size, seen without enhancement in arterial phase (B). Voluminous ascites and splenomegaly developed, due to severe parenchymal atrophy and progressive hepatic dysfunction (B).
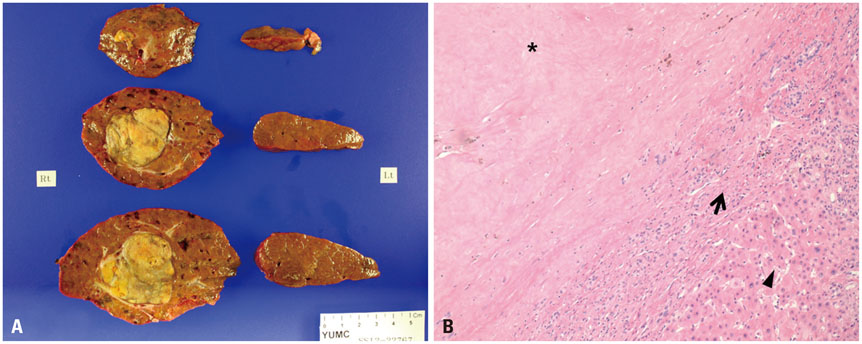
Fig. 3 Gross and microscopic views of liver specimen: note expansile necrotic mass 4.8 cm in size, with diffuse macronodular parenchymal cirrhosis (A). At high magnification, complete necrosis of hepatocellular carcinoma (near asterisk), inflammatory change (near arrow), and normal hepatocytes (near arrowhead) are observed (B; hematoxylin and eosin stain, ×100).
Cited by 1 articles
-
2022 KLCA-NCC Korea practice guidelines for the management of hepatocellular carcinoma
J Liver Cancer. 2023;23(1):1-120. doi: 10.17998/jlc.2022.11.07.
Reference
-
1. Llovet JM, Bustamante J, Castells A, Vilana R, Ayuso Mdel C, Sala M, et al. Natural history of untreated nonsurgical hepatocellular carcinoma: rationale for the design and evaluation of therapeutic trials. Hepatology. 1999; 29:62–67.
Article2. Ando E, Yamashita F, Tanaka M, Tanikawa K. A novel chemotherapy for advanced hepatocellular carcinoma with tumor thrombosis of the main trunk of the portal vein. Cancer. 1997; 79:1890–1896.
Article3. Liang LJ, Hu WJ, Yin XY, Zhou Q, Peng BG, Li DM, et al. Adjuvant intraportal venous chemotherapy for patients with hepatocellular carcinoma and portal vein tumor thrombi following hepatectomy plus portal thrombectomy. World J Surg. 2008; 32:627–631.
Article4. Peng BG, He Q, Li JP, Zhou F. Adjuvant transcatheter arterial chemoembolization improves efficacy of hepatectomy for patients with hepatocellular carcinoma and portal vein tumor thrombus. Am J Surg. 2009; 198:313–318.
Article5. Peng ZW, Guo RP, Zhang YJ, Lin XJ, Chen MS, Lau WY. Hepatic resection versus transcatheter arterial chemoembolization for the treatment of hepatocellular carcinoma with portal vein tumor thrombus. Cancer. 2012; 118:4725–4736.
Article6. Lin DX, Zhang QY, Li X, Ye QW, Lin F, Li LL. An aggressive approach leads to improved survival in hepatocellular carcinoma patients with portal vein tumor thrombus. J Cancer Res Clin Oncol. 2011; 137:139–149.
Article7. Shi J, Lai EC, Li N, Guo WX, Xue J, Lau WY, et al. Surgical treatment of hepatocellular carcinoma with portal vein tumor thrombus. Ann Surg Oncol. 2010; 17:2073–2080.
Article8. Zhou Q, Wang Y, Zhou X, Peng B, Yang J, Liang L, et al. Prognostic analysis for treatment modalities in hepatocellular carcinomas with portal vein tumor thrombi. Asian Pac J Cancer Prev. 2011; 12:2847–2850.9. Choi HJ, Kim DG, Na GH, Hong TH, You YK. Extended criteria for living donor liver transplantation in patients with advanced hepatocellular carcinoma. Transplant Proc. 2012; 44:399–402.
Article10. De Luna W, Sze DY, Ahmed A, Ha BY, Ayoub W, Keeffe EB, et al. Transarterial chemoinfusion for hepatocellular carcinoma as down-staging therapy and a bridge toward liver transplantation. Am J Transplant. 2009; 9:1158–1168.
Article11. Hwang S, Moon DB, Lee SG. Liver transplantation and conventional surgery for advanced hepatocellular carcinoma. Transpl Int. 2010; 23:723–727.
Article12. Chapman WC, Majella Doyle MB, Stuart JE, Vachharajani N, Crippin JS, Anderson CD, et al. Outcomes of neoadjuvant transarterial chemoembolization to downstage hepatocellular carcinoma before liver transplantation. Ann Surg. 2008; 248:617–625.
Article13. Han KH, Seong J, Kim JK, Ahn SH, Lee DY, Chon CY. Pilot clinical trial of localized concurrent chemoradiation therapy for locally advanced hepatocellular carcinoma with portal vein thrombosis. Cancer. 2008; 113:995–1003.
Article14. Lee HS, Choi GH, Choi JS, Kim KS, Han KH, Seong J, et al. Surgical resection after down-staging of locally advanced hepatocellular carcinoma by localized concurrent chemoradiotherapy. Ann Surg Oncol. 2014; 21:3646–3653.
Article15. Mazzaferro V, Regalia E, Doci R, Andreola S, Pulvirenti A, Bozzetti F, et al. Liver transplantation for the treatment of small hepatocellular carcinomas in patients with cirrhosis. N Engl J Med. 1996; 334:693–699.
Article16. Yao FY. Liver transplantation for hepatocellular carcinoma: beyond the Milan criteria. Am J Transplant. 2008; 8:1982–1989.
Article17. Yao FY, Ferrell L, Bass NM, Watson JJ, Bacchetti P, Venook A, et al. Liver transplantation for hepatocellular carcinoma: expansion of the tumor size limits does not adversely impact survival. Hepatology. 2001; 33:1394–1403.
Article18. Toso C, Mentha G, Kneteman NM, Majno P. The place of down-staging for hepatocellular carcinoma. J Hepatol. 2010; 52:930–936.
Article19. Barakat O, Wood RP, Ozaki CF, Ankoma-Sey V, Galati J, Skolkin M, et al. Morphological features of advanced hepatocellular carcinoma as a predictor of downstaging and liver transplantation: an intention-to-treat analysis. Liver Transpl. 2010; 16:289–299.
Article20. Graziadei IW, Sandmueller H, Waldenberger P, Koenigsrainer A, Nachbaur K, Jaschke W, et al. Chemoembolization followed by liver transplantation for hepatocellular carcinoma impedes tumor progression while on the waiting list and leads to excellent outcome. Liver Transpl. 2003; 9:557–563.
Article21. Ravaioli M, Grazi GL, Piscaglia F, Trevisani F, Cescon M, Ercolani G, et al. Liver transplantation for hepatocellular carcinoma: results of down-staging in patients initially outside the Milan selection criteria. Am J Transplant. 2008; 8:2547–2557.
Article22. Di Sandro S, Giacomoni A, Slim A, Lauterio A, Mangoni I, Mihaylov P, et al. Living donor liver transplantation for hepatocellular carcinoma: the impact of neo-adjuvant treatments on the long term results. Hepatogastroenterology. 2012; 59:505–510.23. Gordon-Weeks AN, Snaith A, Petrinic T, Friend PJ, Burls A, Silva MA. Systematic review of outcome of downstaging hepatocellular cancer before liver transplantation in patients outside the Milan criteria. Br J Surg. 2011; 98:1201–1208.
Article24. Lei J, Wang W, Yan L. Downstaging advanced hepatocellular carcinoma to the Milan criteria may provide a comparable outcome to conventional Milan criteria. J Gastrointest Surg. 2013; 17:1440–1446.
Article25. Lau WY, Lai EC. Salvage surgery following downstaging of unresectable hepatocellular carcinoma--a strategy to increase resectability. Ann Surg Oncol. 2007; 14:3301–3309.
Article26. Robertson JM, Lawrence TS, Dworzanin LM, Andrews JC, Walker S, Kessler ML, et al. Treatment of primary hepatobiliary cancers with conformal radiation therapy and regional chemotherapy. J Clin Oncol. 1993; 11:1286–1293.
Article27. Park JY, Ahn SH, Yoon YJ, Kim JK, Lee HW, Lee DY, et al. Repetitive short-course hepatic arterial infusion chemotherapy with high-dose 5-fluorouracil and cisplatin in patients with advanced hepatocellular carcinoma. Cancer. 2007; 110:129–137.
Article28. Park MS, Kim SU, Park JY, Kim DY, Ahn SH, Han KH, et al. Combination treatment of localized concurrent chemoradiation therapy and transarterial chemoembolization in locally advanced hepatocellular carcinoma with intrahepatic metastasis. Cancer Chemother Pharmacol. 2013; 71:165–173.
Article29. Ueshima K, Kudo M, Takita M, Nagai T, Tatsumi C, Ueda T, et al. Hepatic arterial infusion chemotherapy using low-dose 5-fluorouracil and cisplatin for advanced hepatocellular carcinoma. Oncology. 2010; 78:Suppl 1. 148–153.
Article30. Mueller CK, Schultze-Mosgau S. Radiation-induced microenvironments--the molecular basis for free flap complications in the pre-irradiated field? Radiother Oncol. 2009; 93:581–585.
Article31. Heimbach JK, Gores GJ, Haddock MG, Alberts SR, Nyberg SL, Ishitani MB, et al. Liver transplantation for unresectable perihilar cholangiocarcinoma. Semin Liver Dis. 2004; 24:201–207.
Article32. Iwatsuki S, Starzl TE, Sheahan DG, Yokoyama I, Demetris AJ, Todo S, et al. Hepatic resection versus transplantation for hepatocellular carcinoma. Ann Surg. 1991; 214:221–228.
Article33. Ringe B, Pichlmayr R, Wittekind C, Tusch G. Surgical treatment of hepatocellular carcinoma: experience with liver resection and transplantation in 198 patients. World J Surg. 1991; 15:270–285.
Article34. Fujiki M, Aucejo F, Kim R. Adjuvant treatment of hepatocellular carcinoma after orthotopic liver transplantation: do we really need this? Clin Transplant. 2013; 27:169–177.
Article35. Pawarode A, Voravud N, Sriuranpong V, Kullavanijaya P, Patt YZ. Natural history of untreated primary hepatocellular carcinoma: a retrospective study of 157 patients. Am J Clin Oncol. 1998; 21:386–391.36. Yeung YP, Lo CM, Liu CL, Wong BC, Fan ST, Wong J. Natural history of untreated nonsurgical hepatocellular carcinoma. Am J Gastroenterol. 2005; 100:1995–2004.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Liver transplantation for hepatocellular carcinoma with portal vein tumor thrombosis
- Living donor liver transplantation for advanced hepatocellular carcinoma with portal vein tumor thrombosis after concurrent chemoradiation therapy
- Management strategies for advanced hepatocellular carcinoma with portal vein tumor thrombosis
- Concurrent transarterial radioembolization and combination atezolizumab/ bevacizumab treatment of infiltrative hepatocellular carcinoma with portal vein tumor thrombosis: a case report
- Portal flow augmentation using meso-reno-portal anastomosis during liver transplantation with severe portal vein thrombosis
