Yonsei Med J.
2016 Jul;57(4):855-864. 10.3349/ymj.2016.57.4.855.
Prognostic Factors for Recurrence and Progression in Korean Non-Muscle-Invasive Bladder Cancer Patients: A Retrospective, Multi-Institutional Study
- Affiliations
-
- 1Department of Urology, Dongguk University Ilsan Medical Center, Goyang, Korea.
- 2Department of Urology, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Urology, Ajou University College of Medicine, Suwon, Korea.
- 4Department of Urology, Yonsei University College of Medicine, Seoul, Korea.
- 5Department of Urology, The Catholic University College of Medicine, Seoul, Korea.
- 6Department of Urology, Konkuk University College of Medicine, Chungju, Korea.
- 7Department of Urology, Kyungpook National University College of Medicine, Daegu, Korea.
- 8Department of Urology, Hallym University College of Medicine, Chuncheon, Korea.
- 9Department of Urology, Samsung Medical Center, Sungkyunkwan University College of Medicine, Seoul, Korea.
- 10Department of Urology, Kangbuk Samsung Hospital, Sungkyunkwan University College of Medicine, Seoul, Korea.
- 11Department of Urology, Asan Medical Center, Ulsan University College of Medicine, Seoul, Korea.
- 12Department of Urology, Korea University College of Medicine, Seoul, Korea.
- 13Department of Urology, Inha University College of Medicine, Incheon, Korea.
- 14Department of Urology, Chonnam National University College of Medicine, Gwangju, Korea.
- 15Department of Urology, Chonbuk National University College of Medicine, Jeonju, Korea.
- 16Department of Urology, Chungnam National University College of Medicine, Daejeon, Korea.
- 17Department of Urology, Kyung Hee University School of Medicine, Seoul, Korea. hllee61@hanmail.net
- KMID: 2374115
- DOI: http://doi.org/10.3349/ymj.2016.57.4.855
Abstract
- PURPOSE
To identify the prognostic factors related to tumor recurrence and progression in Korean patients with non-muscle-invasive bladder cancer (NMIBC).
MATERIALS AND METHODS
Data were collected and analyzed for 2412 NMIBC patients from 15 centers who were initially diagnosed after transurethral resection of bladder tumor (TURBT) from January 2006 to December 2010. Using univariable and multivariable Cox proportional hazards models, the prognostic value of each variable was evaluated for the time to first recurrence and progression.
RESULTS
With a median follow-up duration of 37 months, 866 patients (35.9%) experienced recurrence, and 137 (5.7%) experienced progression. Patients with recurrence had a median time to the first recurrence of 10 months. Multivariable analysis conducted in all patients revealed that preoperative positive urine cytology (PUC) was independently associated with worse recurrence-free survival [RFS; hazard ratio (HR) 1.56; p<0.001], and progression-free survival (PFS; HR 1.56; p=0.037). In particular, on multivariable analysis conducted for the high-risk group (T1 tumor/high-grade Ta tumor/carcinoma in situ), preoperative PUC was an independent predictor of worse RFS (HR 1.73; p<0.001) and PFS (HR 1.96; p=0.006). On multivariable analysis in patients with T1 high-grade (T1HG) cancer (n=684), better RFS (HR 0.75; p=0.033) and PFS (HR 0.33; p<0.001) were observed in association with the administration of intravesical Bacillus Calmette-Guérin (BCG) induction therapy.
CONCLUSION
A preoperative PUC result may adversely affect RFS and PFS, particularly in high-risk NMIBC patients. Of particular note, intravesical BCG induction therapy should be administered as an adjunct to TURBT in order to improve RFS and PFS in patients with T1HG cancer.
MeSH Terms
Figure
-
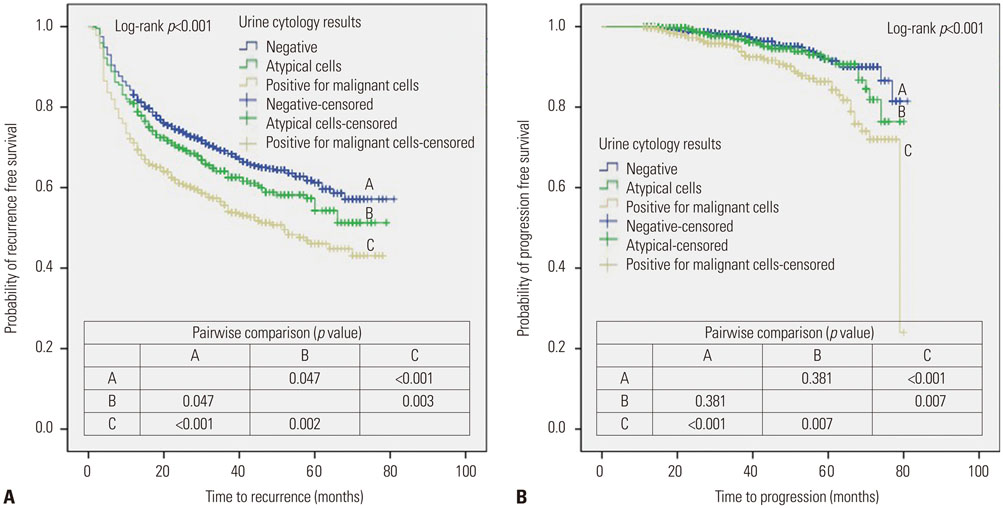
Fig. 1 Kaplan-Meier plots for recurrence-free survival (A) and progression-free survival (B) stratified by urine cytology result for the entire study cohort.

Fig. 2 Kaplan-Meier plots for recurrence-free survival (A) and progression-free survival (B) according to risk stratification.

Fig. 3 Kaplan-Meier plots for recurrence-free survival (A) and progression-free survival (B) stratified by induction intravesical BCG for patients with T1 high-grade urothelial carcinoma. BCG, Bacillus Calmette-Guérin.
Reference
-
1. Siegel R, Ma J, Zou Z, Jemal A. Cancer statistics, 2014. CA Cancer J Clin. 2014; 64:9–29.
Article2. Jung KW, Won YJ, Kong HJ, Oh CM, Lee DH, Lee JS. Prediction of cancer incidence and mortality in Korea, 2014. Cancer Res Treat. 2014; 46:124–130.
Article3. Babjuk M, Burger M, Zigeuner R, Shariat SF, van Rhijn BW, Compérat E, et al. EAU guidelines on non-muscle-invasive urothelial carcinoma of the bladder: update 2013. Eur Urol. 2013; 64:639–653.
Article4. Burger M, Oosterlinck W, Konety B, Chang S, Gudjonsson S, Pruthi R, et al. ICUD-EAU International Consultation on Bladder Cancer 2012: non-muscle-invasive urothelial carcinoma of the bladder. Eur Urol. 2013; 63:36–44.
Article5. Segal R, Yafi FA, Brimo F, Tanguay S, Aprikian A, Kassouf W. Prognostic factors and outcome in patients with T1 high-grade bladder cancer: can we identify patients for early cystectomy? BJU Int. 2012; 109:1026–1030.
Article6. Chamie K, Litwin MS, Bassett JC, Daskivich TJ, Lai J, Hanley JM, et al. Recurrence of high-risk bladder cancer: a population-based analysis. Cancer. 2013; 119:3219–3227.
Article7. Lammers RJ, Witjes WP, Hendricksen K, Caris CT, Janzing-Pastors MH, Witjes JA. Smoking status is a risk factor for recurrence after transurethral resection of non-muscle-invasive bladder cancer. Eur Urol. 2011; 60:713–720.
Article8. Palou J, Sylvester RJ, Faba OR, Parada R, Peña JA, Algaba F, et al. Female gender and carcinoma in situ in the prostatic urethra are prognostic factors for recurrence, progression, and disease-specific mortality in T1G3 bladder cancer patients treated with bacillus Calmette-Guérin. Eur Urol. 2012; 62:118–125.
Article9. Kluth LA, Fajkovic H, Xylinas E, Crivelli JJ, Passoni N, Rouprêt M, et al. Female gender is associated with higher risk of disease recurrence in patients with primary T1 high-grade urothelial carcinoma of the bladder. World J Urol. 2013; 31:1029–1036.
Article10. Sfakianos JP, Kim PH, Hakimi AA, Herr HW. The effect of restaging transurethral resection on recurrence and progression rates in patients with nonmuscle invasive bladder cancer treated with intravesical Bacillus Calmette-Guérin. J Urol. 2014; 191:341–345.
Article11. Shindo T, Masumori N, Kitamura H, Tanaka T, Fukuta F, Hasegawa T, et al. Clinical significance of definite muscle layer in TUR specimen for evaluating progression rate in T1G3 bladder cancer: multi-center retrospective study by the Sapporo Medical University Urologic Oncology Consortium (SUOC). World J Urol. 2014; 32:1281–1285.
Article12. Zachos I, Tzortzis V, Mitrakas L, Samarinas M, Karatzas A, Gravas S, et al. Tumor size and T stage correlate independently with recurrence and progression in high-risk non-muscle-invasive bladder cancer patients treated with adjuvant BCG. Tumour Biol. 2014; 35:4185–4189.
Article13. Gontero P, Sylvester R, Pisano F, Joniau S, Vander Eeckt K, Serretta V, et al. Prognostic factors and risk groups in T1G3 non-muscle-invasivebladder cancer patients initially treated with Bacillus Calmette-Guérin: results of a retrospective multicenter study of 2451 patients. Eur Urol. 2015; 67:74–82.14. Seo KW, Kim BH, Park CH, Kim CI, Chang HS. The efficacy of the EORTC scoring system and risk tables for the prediction of recurrence and progression of non-muscle-invasive bladder cancer after intravesical Bacillus Calmette-Guerin instillation. Korean J Urol. 2010; 51:165–170.
Article15. Fernandez-Gomez J, Madero R, Solsona E, Unda M, Martinez-Piñeiro L, Ojea A, et al. The EORTC tables overestimate the risk of recurrence and progression in patients with non-muscle-invasive bladder cancer treated with Bacillus Calmette-Guérin: external validation of the EORTC risk tables. Eur Urol. 2011; 60:423–430.
Article16. Hernández V, De La Peña E, Martin MD, Blázquez C, Diaz FJ, Llorente C. External validation and applicability of the EORTC risk tables for non-muscle-invasive bladder cancer. World J Urol. 2011; 29:409–414.
Article17. Fernandez-Gomez J, Madero R, Solsona E, Unda M, Martinez-Piñeiro L, Gonzalez M, et al. Predicting nonmuscle invasive bladder cancer recurrence and progression in patients treated with Bacillus Calmette-Guerin: the CUETO scoring model. J Urol. 2009; 182:2195–2203.
Article18. Sylvester RJ, Oosterlinck W, van der Meijden AP. A single immediate postoperative instillation of chemotherapy decreases the risk of recurrence in patients with stage Ta T1 bladder cancer: a meta-analysis of published results of randomized clinical trials. J Urol. 2004; 171(6 Pt 1):2186–2190.
Article19. Huncharek M, McGarry R, Kupelnick B. Impact of intravesical chemotherapy on recurrence rate of recurrent superficial transitional cell carcinoma of the bladder: results of a meta-analysis. Anticancer Res. 2001; 21:765–769.20. Sylvester RJ, Oosterlinck W, Witjes JA. The schedule and duration of intravesical chemotherapy in patients with non-muscle-invasive bladder cancer: a systematic review of the published results of randomized clinical trials. Eur Urol. 2008; 53:709–719.
Article21. Lavallée LT, Fergusson D, Dahm P, Scales CD Jr, Witiuk K, Breau RH. Diagnostic tests in urology: urine cytology. BJU Int. 2012; 110(11 Pt C):E789–E791.
Article22. Yafi FA, Brimo F, Auger M, Aprikian A, Tanguay S, Kassouf W. Is the performance of urinary cytology as high as reported historically? A contemporary analysis in the detection and surveillance of bladder cancer. Urol Oncol. 2014; 32:27.e1–27.e6.
Article23. Kobayashi Y, Saika T, Miyaji Y, Saegusa M, Arata R, Akebi N, et al. Preoperative positive urine cytology is a risk factor for subsequent development of bladder cancer after nephroureterectomy in patients with upper urinary tract urothelial carcinoma. World J Urol. 2012; 30:271–275.
Article24. Lodde M, Mayr R, Martini T, Comploj E, Palermo S, Trenti E, et al. Positive urine cytology and carcinoma in situ prior to second transurethral resection of the bladder correlate with positive second resection histology and the need for subsequent cystectomy. World J Urol. 2012; 30:841–846.
Article25. Koga F, Kobayashi S, Fujii Y, Ishioka J, Yokoyama M, Nakanishi Y, et al. Significance of positive urine cytology on progression and cancer-specific mortality of non--muscle-invasive bladder cancer. Clin Genitourin Cancer. 2014; 12:e87–e93.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Predicting Recurrence and Progession of Non Muscle Invasive Urothelial Cell Carcinoma of Bladder by Clinical and Pathological Prognostic Factors
- Predictive Value of Urinary Cytology in the Recurrence and the Progression of Superficial Bladder Cancer
- Clinical Prognostic Factors for Radical Cystectomy in Bladder Cancer
- Multivariate Analysis of the Prognostic Significance of Resection Weight after Transurethral Resection of Bladder Tumor for Non-Muscle-Invasive Bladder Cancer
- Autophagy and urothelial carcinoma of the bladder: A review
