Yonsei Med J.
2016 May;57(3):658-663. 10.3349/ymj.2016.57.3.658.
Waist-to-Height Ratio as an Index for Cardiometabolic Risk in Adolescents: Results from the 1998-2008 KNHANES
- Affiliations
-
- 1Department of Pediatrics, National Health Insurance Service Ilsan Hospital, Goyang, Korea.
- 2Center for International Health Research, Rhode Island Hospital, The Warren Alpert Medical School of Brown University, Providence, RI, USA.
- 3Department of Pediatrics, The Warren Alpert Medical School of Brown University, Providence, RI, USA.
- 4Department of Pediatrics, Sanggye Paik Hospital, College of Medicine, Inje University, Seoul, Korea. pmj@paik.ac.kr
- 5Department of Pediatrics, College of Medicine, CHA University, Seongnam, Korea. pedyoo@cha.ac.kr
- KMID: 2374086
- DOI: http://doi.org/10.3349/ymj.2016.57.3.658
Abstract
- PURPOSE
To describe the relationship between the waist-to-height ratio (WHtR) and cardiometabolic risk factors (CMRFs) and to evaluate the validity of WHtR in identifying adolescents with metabolic syndrome.
MATERIALS AND METHODS
We analyzed data from a pooled population of 4068 adolescents aged 10-19 years from the Korean National Health and Nutrition Examination Surveys conducted between 1998 and 2008. Overweight individuals were defined by body mass index (BMI) ≥85th percentile. Those with at least 2 CMRFs among hypertension, hyperglycemia, hypertriglyceridemia, and decreased high-density lipoprotein cholesterol (HDL-C) were classified as having multiple CMRFs.
RESULTS
WHtR was significantly related to systolic blood pressure, HDL-C, and triglycerides in both non-overweight and overweight adolescents (all p<0.01). Among overweight adolescents, the area under the curve (AUC) for WHtR in identifying multiple CMRFs was significantly greater than that for BMI (p=0.014). Metabolic syndrome was more common in overweight adolescents with a WHtR of ≥0.5 than in those with a WHtR of <0.5 (p<0.001). In non-overweight adolescents, the prevalences of multiple CMRFs (p=0.001) and metabolic syndrome (p<0.001) were higher in those with a WHtR of ≥0.5 than in those with a WHtR of <0.5. Among those without central obesity, the prevalence of multiple CMRFs was higher in those with a WHtR of ≥0.5 than in those with a WHtR of <0.5 (p=0.021).
CONCLUSION
WHtR is a simple and valid index for identifying adolescents with increased cardiometabolic risk and is related to CMRFs even in non-overweight adolescents. In adolescents already screened via BMI and waist circumference (WC), WHtR seems to be of additional help in discriminating those at higher cardiometabolic risk.
Keyword
MeSH Terms
-
Adolescent
Blood Pressure/physiology
*Body Height
Body Mass Index
Cardiovascular Diseases/*epidemiology
Child
Cholesterol, HDL/blood
Female
Humans
Hypertension/complications/epidemiology
Male
Metabolic Syndrome X/*epidemiology
Nutrition Surveys
Obesity, Abdominal/complications/*epidemiology
Republic of Korea/epidemiology
Risk Factors
Triglycerides/blood
*Waist Circumference/physiology
*Waist-Height Ratio
Young Adult
Cholesterol, HDL
Triglycerides
Figure
-
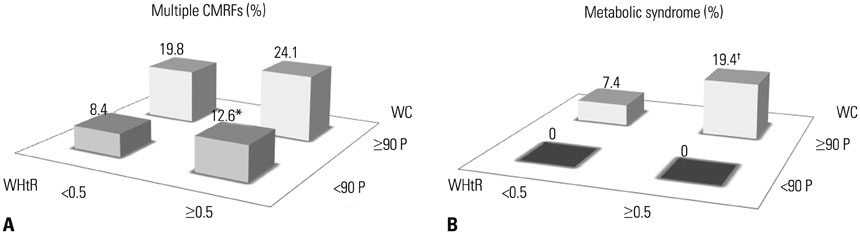
Fig. 1 The prevalence of multiple CMRFs (A) and metabolic syndrome (B) in overweight (BMI ≥85 P) and non-overweight (BMI <85 P) adolescents further stratified by WHtR. *p<0.05 vs. BMI <85 P/WHtR <0.5 group, †p<0.05 vs. BMI ≥85 P/WHtR <0.5 group. WHtR, waist to height ratio; BMI, body mass index; CMRFs, cardiometabolic risk factors.
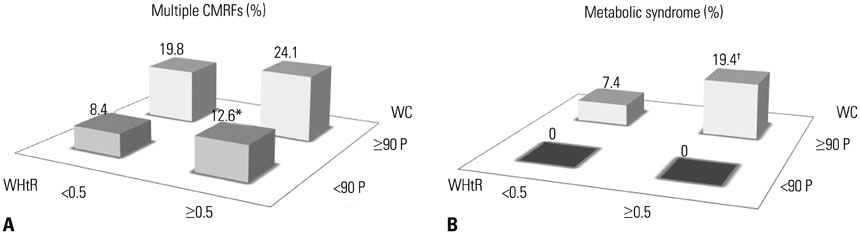
Fig. 2 The prevalence of multiple CMRFs (A) and metabolic syndrome (B) in adolescents those with central obesity (WC ≥90 P) and without central obesity (WC <90 P) further stratified by WHtR. *p<0.05 vs. WC <90 P/WHtR <0.5 group, †p<0.05 vs. WC ≥90 P/WHtR <0.5 group. WHtR, waist to height ratio; WC, waist circumference; CMRFs, cardiometabolic risk factors.
Reference
-
1. Duncan GE, Li SM, Zhou XH. Prevalence and trends of a metabolic syndrome phenotype among us Adolescents, 1999-2000. Diabetes Care. 2004; 27:2438–2443.
Article2. Han JC, Lawlor DA, Kimm SY. Childhood obesity. Lancet. 2010; 375:1737–1748.
Article3. Expert Panel on Detection, Evaluation, and Treatment of High Blood Cholesterol in Adults. Executive Summary of The Third Report of The National Cholesterol Education Program (NCEP) Expert Panel on Detection, Evaluation, And Treatment of High Blood Cholesterol In Adults (Adult Treatment Panel III). JAMA. 2001; 285:2486–2497.4. Park MJ, Boston BA, Oh M, Jee SH. Prevalence and trends of metabolic syndrome among Korean adolescents: from the Korean NHANES survey, 1998-2005. J Pediatr. 2009; 155:529–534.
Article5. Morrison JA, Friedman LA, Wang P, Glueck CJ. Metabolic syndrome in childhood predicts adult metabolic syndrome and type 2 diabetes mellitus 25 to 30 years later. J Pediatr. 2008; 152:201–206.
Article6. WHO Expert Consultation. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004; 363:157–163.7. Zimmet P, Magliano D, Matsuzawa Y, Alberti G, Shaw J. The metabolic syndrome: a global public health problem and a new definition. J Atheroscler Thromb. 2005; 12:295–300.
Article8. Yajnik CS, Yudkin JS. The Y-Y paradox. Lancet. 2004; 363:163.
Article9. Lee CM, Huxley RR, Wildman RP, Woodward M. Indices of abdominal obesity are better discriminators of cardiovascular risk factors than BMI: a meta-analysis. J Clin Epidemiol. 2008; 61:646–653.
Article10. Spolidoro JV, Pitrez Filho ML, Vargas LT, Santana JC, Pitrez E, Hauschild JA, et al. Waist circumference in children and adolescents correlate with metabolic syndrome and fat deposits in young adults. Clin Nutr. 2013; 32:93–97.
Article11. Khoury M, Manlhiot C, McCrindle BW. Role of the waist/height ratio in the cardiometabolic risk assessment of children classified by body mass index. J Am Coll Cardiol. 2013; 62:742–751.
Article12. Ashwell M, Hsieh SD. Six reasons why the waist-to-height ratio is a rapid and effective global indicator for health risks of obesity and how its use could simplify the international public health message on obesity. Int J Food Sci Nutr. 2005; 56:303–307.
Article13. Maffeis C, Banzato C, Talamini G. Obesity Study Group of the Italian Society of Pediatric Endocrinology and Diabetology. Waist-to-height ratio, a useful index to identify high metabolic risk in overweight children. J Pediatr. 2008; 152:207–213.
Article14. Zimmet P, Alberti KG, Kaufman F, Tajima N, Silink M, Arslanian S, et al. The metabolic syndrome in children and adolescents - an IDF consensus report. Pediatr Diabetes. 2007; 8:299–306.
Article15. Moon JS, Lee SY, Nam CM, Choi JM, Choe BK, Seo JW, et al. 2007 Korean national growth charts: review of developmental process and an outlook. Korean J Pediatr. 2008; 51:1–25.
Article16. Lee SY, Park HS, Kim DJ, Han JH, Kim SM, Cho GJ, et al. Appropriate waist circumference cutoff points for central obesity in Korean adults. Diabetes Res Clin Pract. 2007; 75:72–80.
Article17. Akobeng AK. Understanding diagnostic tests 3: receiver operating characteristic curves. Acta Paediatr. 2007; 96:644–647.
Article18. Saydah S, Bullard KM, Imperatore G, Geiss L, Gregg EW. Cardiometabolic risk factors among US adolescents and young adults and risk of early mortality. Pediatrics. 2013; 131:e679–e686.
Article19. Gil JH, Lee MN, Lee HA, Park HS, Seo JW. Usefulness of the waist circumference-to-height ratio in screening for obesity in Korean children and adolescents. Korean J Pediatr Gastroenterol Nutr. 2010; 13:180–192.
Article20. Sung RY, So HK, Choi KC, Nelson EA, Li AM, Yin JA, et al. Waist circumference and waist-to-height ratio of Hong Kong Chinese children. BMC Public Health. 2008; 8:324.
Article21. Hsieh SD, Yoshinaga H. Do people with similar waist circumference share similar health risks irrespective of height? Tohoku J Exp Med. 1999; 188:55–60.
Article22. Kromeyer-Hauschild K, Neuhauser H, Schaffrath Rosario A, Schienkiewitz A. Abdominal obesity in German adolescents defined by waist-to-height ratio and its association to elevated blood pressure: the KiGGS study. Obes Facts. 2013; 6:165–175.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Waist-to-height ratio as a screening tool for obesity and cardiometabolic risk
- Waist-height ratio and body mass index as indicators of obesity and cardiometabolic risk in Korean children and adolescents
- Reference Values for Waist Circumference and Waist–Height Ratio in Korean Children and Adolescents
- The Comparison of Efficacy of Obesity Indices for Screening Metabolic Risk Factors Among Adults In Jeju Island
- Waist-to-height Ratio, a Simple and Practical Index for Screening of Adolescent Metabolic Syndrome Aged 17~19 Years
