Management of Ventilatory Insufficiency in Neuromuscular Patients Using Mechanical Ventilator Supported by the Korean Government
- Affiliations
-
- 1Department of Rehabilitation Medicine, Pulmonary Rehabilitation Center, Gangnam Severance Hospital, Rehabilitation Institute of Neuromuscular Disease, Yonsei University College of Medicine, Seoul, Korea. kswoong@yuhs.ac
- KMID: 2373709
- DOI: http://doi.org/10.3346/jkms.2016.31.6.976
Abstract
- Since 2001, financial support has been provided for all patients with neuromuscular disease (NMD) who require ventilatory support due to the paralysis of respiratory muscles in Korea. The purpose of this study was to identify ventilator usage status and appropriateness in these patients. We included 992 subjects with rare and incurable NMD registered for ventilator rental fee support. From 21 February 2011 to 17 January 2013, ventilator usage information, regular follow-up observation, and symptoms of chronic hypoventilation were surveyed by phone. Home visits were conducted for patients judged by an expert medical team to require medical examination. Abnormal ventilatory status was assessed by respiratory evaluation. Chronic respiratory insufficiency symptoms were reported by 169 of 992 subjects (17%), while 565 subjects (57%) did not receive regular respiratory evaluation. Ventilatory status was abnormal in 102 of 343 home-visit subjects (29.7%). Although 556 subjects (56%) reported 24-hour ventilator use, only 458 (46%) had an oxygen saturation monitoring device, and 305 (31%) performed an airstacking exercise. A management system that integrates ventilator usage monitoring, counselling and advice, and home visits for patients who receive ventilator support could improve the efficiency of the ventilator support project.
MeSH Terms
Figure
-
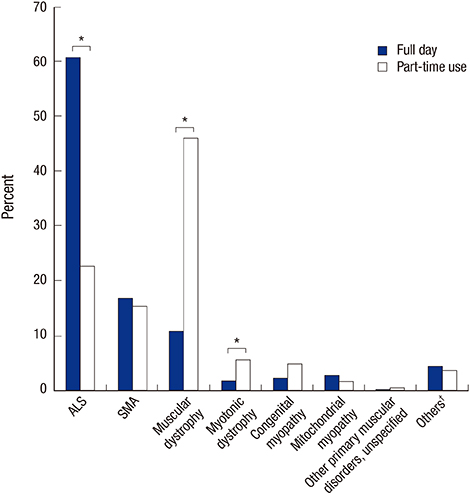
Fig. 1 Percentage of time of the daily ventilator use for each disease. ALS, amyotrophic lateral sclerosis; SMA, spinal muscular atrophy; †This group includes hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease. *Statistically significant P value < 0.05;

Fig. 2 Percentage of type of ventilator use for each disease. IPPV, invasive positive pressure ventilation; NIPPV, non-invasive intermittent positive pressure ventilator; ALS, amyotrophic lateral sclerosis; SMA, spinal muscular atrophy. *Statistically significant P value < 0.05; †This group includes hereditary ataxia, myasthenia gravis, multiple sclerosis, Charcot-Marie-Tooth disease, Guillain-Barre syndrome, mucopolysaccharidosis, Pompe disease, and Creutzfeldt-Jakob disease.

Fig. 3 A number of patients with regular follow-up observation and respiratory evaluation. f/u, follow-up; +, yes; -, no.
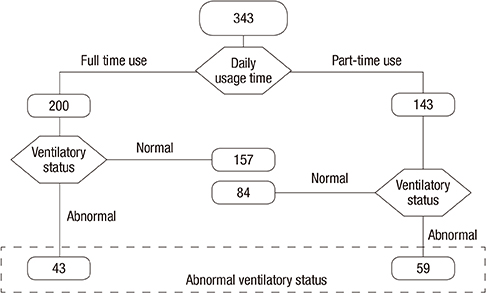
Fig. 4 Ventilatory status of the subjects visited at home.
Reference
-
1. Gibson GJ, Pride NB, Davis JN, Loh LC. Pulmonary mechanics in patients with respiratory muscle weakness. Am Rev Respir Dis. 1977; 115:389–395.2. Griggs RC, Donohoe KM, Utell MJ, Goldblatt D, Moxley RT 3rd. Evaluation of pulmonary function in neuromuscular disease. Arch Neurol. 1981; 38:9–12.3. Lynn DJ, Woda RP, Mendell JR. Respiratory dysfunction in muscular dystrophy and other myopathies. Clin Chest Med. 1994; 15:661–674.4. Schramm CM. Current concepts of respiratory complications of neuromuscular disease in children. Curr Opin Pediatr. 2000; 12:203–207.5. Smith PE, Calverley PM, Edwards RH, Evans GA, Campbell EJ. Practical problems in the respiratory care of patients with muscular dystrophy. N Engl J Med. 1987; 316:1197–1205.6. Kang SW, Park JH, Ryu HH, Kang YS, Moon JH. Non-invasive mechanical ventilator care for the patients with advanced neuromuscular disease. J Korean Acad Rehabil Med. 2004; 28:71–77.7. Misuri G, Lanini B, Gigliotti F, Iandelli I, Pizzi A, Bertolini MG, Scano G. Mechanism of CO2 retention in patients with neuromuscular disease. Chest. 2000; 117:447–453.8. Kim DH, Kang SW, Kim W, Lee SC, Yoo TW, Moon JH. Follow up Survey of Non-invasive intermittent positive pressure ventilatory support in patients with neuromuscular diseases. J Korean Acad Rehabil Med. 2007; 31:427–433.9. Kim DH, Kang SW, Choi W, Moon JH, Baek JH, Choi SH, Park JH, Shin YB, Seo JH. A research on the management of ventilatory insufficiency in patients with neuromuscular diseases. J Korean Acad Rehabil Med. 2010; 34:347–354.10. Simonds AK, Muntoni F, Heather S, Fielding S. Impact of nasal ventilation on survival in hypercapnic Duchenne muscular dystrophy. Thorax. 1998; 53:949–952.11. Bach JR, Alba AS. Management of chronic alveolar hypoventilation by nasal ventilation. Chest. 1990; 97:52–57.12. Bach JR. Amyotrophic lateral sclerosis: predictors for prolongation of life by noninvasive respiratory aids. Arch Phys Med Rehabil. 1995; 76:828–832.13. Kim JY, Min Y, Kim MS, Kim JS, Kim HL, Shin HI. A survey of respiratory care in amyotrophic lateral sclerosis patients using non-invasive ventilatory support. J Korean Acad Rehabil Med. 2010; 34:49–53.14. Rose L, McKim DA, Katz SL, Leasa D, Nonoyama M, Pedersen C, Goldstein RS, Road JD, Amin R, Avendano M, et al. Home mechanical ventilation in Canada: a national survey. Respir Care. 2015; 60:695–704.15. Kang SW, Bach JR. Maximum insufflation capacity. Chest. 2000; 118:61–65.16. Kang SW, Cho DH, Lee SC, Moon JH, Park YG, Song NK, Lee SH. Clinical implication of air stacking exercise in patients with neuromuscular diseases. J Korean Acad Rehabil Med. 2007; 31:346–350.17. Simonds AK, Elliott MW. Outcome of domiciliary nasal intermittent positive pressure ventilation in restrictive and obstructive disorders. Thorax. 1995; 50:604–609.18. Lloyd-Owen SJ, Donaldson GC, Ambrosino N, Escarabill J, Farre R, Fauroux B, Robert D, Schoenhofer B, Simonds AK, Wedzicha JA. Patterns of home mechanical ventilation use in Europe: results from the Eurovent survey. Eur Respir J. 2005; 25:1025–1031.19. Garner DJ, Berlowitz DJ, Douglas J, Harkness N, Howard M, McArdle N, Naughton MT, Neill A, Piper A, Yeo A, et al. Home mechanical ventilation in Australia and New Zealand. Eur Respir J. 2013; 41:39–45.20. Bach JR, Bianchi C, Aufiero E. Oximetry and indications for tracheotomy for amyotrophic lateral sclerosis. Chest. 2004; 126:1502–1507.21. Sancho J, Servera E, Díaz J, Marín J. Efficacy of mechanical insufflation-exsufflation in medically stable patients with amyotrophic lateral sclerosis. Chest. 2004; 125:1400–1405.22. Cheng G, Bach JR. Avoidance of tracheostomy in patients with neuromuscular disease. Chron Respir Dis. 2008; 5:243.23. Soudon P, Steens M, Toussaint M. A comparison of invasive versus noninvasive full-time mechanical ventilation in Duchenne muscular dystrophy. Chron Respir Dis. 2008; 5:87–93.24. Nauffal D, Doménech R, Martínez García MA, Compte L, Macián V, Perpiñá M. Noninvasive positive pressure home ventilation in restrictive disorders: outcome and impact on health-related quality of life. Respir Med. 2002; 96:777–783.25. Radunovic A, Annane D, Rafiq MK, Mustfa N. Mechanical ventilation for amyotrophic lateral sclerosis/motor neuron disease. Cochrane Database Syst Rev. 2013; 3:CD004427.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Noninvasive Respiratory Management of Patients With Neuromuscular Disease
- Non-invasive Mechanical Ventilator Care for the Patients with Advanced Neuromuscular Disease
- Quality of Life in Patients with Neuromuscular Disease Using Mechanical Ventilatory Support
- Home Mechanical Ventilation of Pediatric Patients
- New Modes of Ventilation for Neonates
