Clinicopathological Features of Upper Third Gastric Cancer during a 21-Year Period (Single Center Analysis)
- Affiliations
-
- 1Department of Surgery, Seoul National University College of Medicine, Seoul, Korea. hkyang@snu.ac.kr
- 2Cancer Research Institute, Seoul National University College of Medicine, Seoul, Korea.
- 3Department of Pathology, Seoul National University College of Medicine, Seoul, Korea.
- 4Department of Surgery, Federal University of Sao Paulo, Sao Paulo, Brasil.
Abstract
- PURPOSE
The aim of this study was to determine proportions of upper third gastric cancer (UTG) among all gastric cancers and analyze clinicopathological features of the disease.
MATERIALS AND METHODS
The medical records of 12,300 patients who underwent gastric surgery between 1986 and 2006 at Seoul National University Hospital (SNUH) were retrospectively reviewed. Clinicopathological features of 1,260 patients with UTG and 9,929 patients with middle or lower third gastric cancer (MLG) were compared, and annual proportions of UTG were evaluated.
RESULTS
The proportion of patients with UTG rapidly increased from 2.6% in 1986 to 12.5% in 1992. However, linear regression analysis showed that the rate of increase was reduced (0.21%/year) after 1992 (12.5% to 14.2% from 1992 to 2006). Compared with the MLG group, the UTG group had a lower proportion of (22.3% vs. 39.7%, P<0.001) and a greater proportion of stage III/IV disease (39.4% vs. 31.7%, P<0.001). The UTG group also had larger tumors than the MLG group in stages I/II and III (3.5 cm/5.3 cm/6.5 cm vs. 3.2 cm/5.0 cm/5.8 cm, P=0.020/0.028 /<0.001), a higher proportion of undifferentiated cancer (63.1% vs. 53.7%, P<0.001), and less intestinal Lauren's type (38.8% vs. 47.4%, P<0.001). The 5-year survival rate of the UTG group was significantly lower than that of the MLG group in stages I/II and III (85.6%/63.1%/34.2% vs. 91.6%/ 69.2%/44.7%, P<0.001/0.028/0.006).
CONCLUSIONS
The proportion of UTGs has increased over the last two decades at SNUH, but the rate of increase has been greatly reduced since 1992. The UTG group showed a poorer prognosis compared with the MLG group in stages I/II and III.
Keyword
MeSH Terms
Figure
-
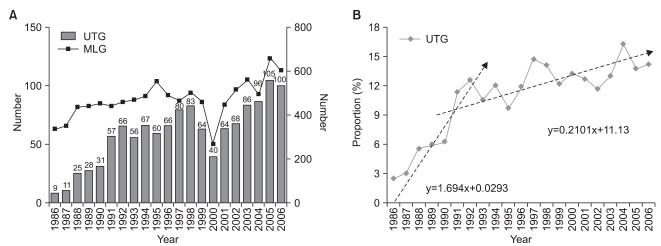
Fig. 1 Chronological changes in gastric cancer patient numbers based on tumor location. (A) Annual number of UTG and MLG at SNUH. UTG was 2.6% (9 patients) in 1986 and rapidly increased to 12.5% (66 patients) in 1992. It reached a peak of 16.2% (96 patients) in 2004. A temporary drop in the rate to 12.5% (40 patients) was observed in 2000, which may be related to a medical strike at the time in Korea for separating medical practice and pharmaceutical dispensing system. (B) Estimated increase in the rates of UTG by linear regression analysis. Before 1992, UTG had been increasing at the rate of 1.69% per year (P<0.001, R2=0.913); since 1992, the rate has reduced at 0.21% per year (P=0.028, R2=0.321). UTG = upper third gastric cancer; MLG = middle or lower third gastric cancer; SNUH = Seoul National University Hospital.
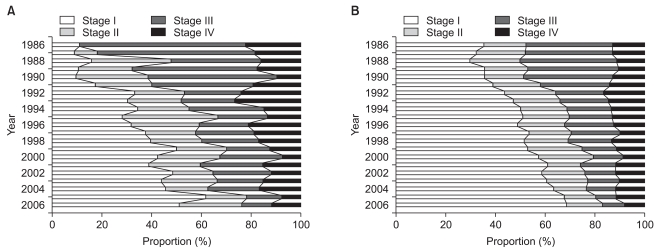
Fig. 2 Chronological changes in gastric cancer stages based on the tumor location. The proportion of stage I and II cancer increased in both groups, whereas the proportion of stage III and IV decreased; it is not clear whether this represents a real increase in the prevalence of EGC or is simply the result of greater diagnoses due to increased health screening. (A) Annual TNM stage distribution in UTG. (B) Annual TNM stage distribution in MLG. EGC = early gastric cancer; MLG = middle or lower third gastric cancer.
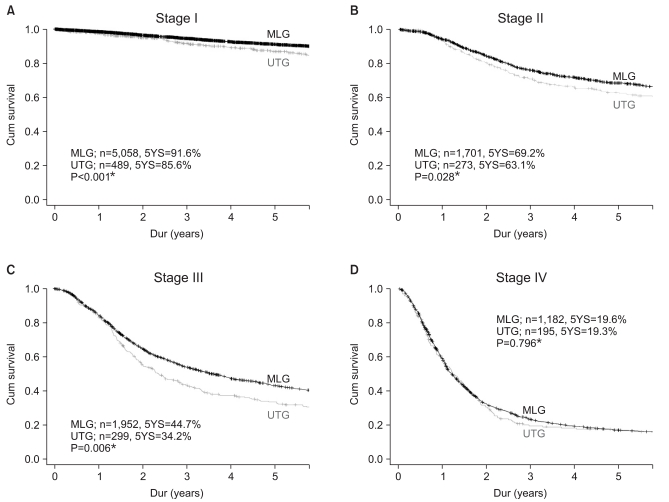
Fig. 3 Survival curve of gastric cancer in each stage based on the tumor locaton. Five-year survival rates in UTG were significantly lower compared with MLG in stage I, II, and III; there was no significant difference in stage IV. (A) Stage I. (B) Stage II. (C) Stage III. (D) Stage IV. MLG = middle or lower third gastric cancer; UTG = upper third gastric cancer; YS = year survival rate. ‡P<0.05, statistically significant.
Reference
-
1. Parkin DM, Bray F, Ferlay J, Pisani P. Global cancer statistics, 2002. CA Cancer J Clin. 2005; 55:74–108. PMID: 15761078.
Article2. Hassan HA, Sharma VK, Raufman JP. Changing trends in gastric carcinoma at a university medical center: a twelve-year retrospective analysis. J Clin Gastroenterol. 2001; 32:37–40. PMID: 11154167.3. Blaser MJ, Saito D. Trends in reported adenocarcinomas of the oesophagus and gastric cardia in Japan. Eur J Gastroenterol Hepatol. 2002; 14:107–113. PMID: 11981333.
Article4. Zhou Y, Zhang Z, Zhang Z, Wu J, Ren D, Yan X, et al. A rising trend of gastric cardia cancer in Gansu Province of China. Cancer Lett. 2008; 269:18–25. PMID: 18501504.
Article5. Ryu KW, Kim CS, Goo BH. Clinicopathologic characteristics of and prognosis for proximal gastric carcinomas. J Korean Surg Soc. 2000; 59:223–228.6. Park MW, Bae JM, Kim SW, Kim SW, Song SK. Annual change of clinicopathologic characteristics after radical gastrectomy due to gastric cancer. J Korean Surg Soc. 2009; 77:88–95.
Article7. Yang HK. The Information Committee of the Korean Gastric Cancer Association. Current status of clinical practice for gastric cancer patients in Korea. J Korean Gastric Cancer Assoc. 2004; 4:95–108.8. Bruno L, Nesi G, Montinaro F, Carassale G, Lassig R, Boddi V, et al. Clinicopathologic findings and results of surgical treatment in cardiac adenocarcinoma. J Surg Oncol. 2000; 74:33–35. PMID: 10861606.
Article9. Talamonti MS, Kim SP, Yao KA, Wayne JD, Feinglass J, Bennett CL, et al. Surgical outcomes of patients with gastric carcinoma: the importance of primary tumor location and microvessel invasion. Surgery. 2003; 134:720–727. PMID: 14605635.
Article10. Kim DY, Joo JK, Ryu SY, Park YK, Kim YJ, Kim SK. Clinicopathological characteristics and prognosis of carcinoma of the gastric cardia. Dig Surg. 2006; 23:313–318. PMID: 17164543.
Article11. Kunisaki C, Akiyama H, Nomura M, Matsuda G, Otsuka Y, Ono H, et al. Surgical outcomes for early gastric cancer in the upper third of the stomach. J Am Coll Surg. 2005; 200:15–19. PMID: 15631915.
Article12. Kim WH, Park CK, Kim YB, Kim YW, Kim HG, Bae HI, et al. A standardized pathology report for gastric cancer. Korean J Pathol. 2005; 39:106–113.13. Nakamura K, Sugano H, Takagi K. Carcinoma of the stomach in incipient phase: its histogenesis and histological appearances. Gann. 1968; 59:251–258. PMID: 5726267.14. Lauren P. The two histological main types of gastric carcinoma: diffuse and so-called intestinal-type carcinoma. an attempt at a histo-clinical classification. Acta Pathol Microbiol Scand. 1965; 64:31–49. PMID: 14320675.15. Tamura G, Sato K, Akiyama S, Tsuchiya T, Endoh Y, Usuba O, et al. Molecular characterization of undifferentiated-type gastric carcinoma. Lab Invest. 2001; 81:593–598. PMID: 11304579.
Article16. Frederick LG, Charles MB, David IP, Daniel GH, Irvin DF, Monica M, April GF, editors. AJCC Cancer Staging Manual. Vol 1. 2002. 6th ed. New York: Springer-Verlag.17. The Information Committee of the Korean Gastric Cancer Association. 2004 nationwide gastric cancer report in Korea. J Korean Gastric Cancer Assoc. 2007; 7:47–54.18. September 1, 2010. Accessed http://www.kgca-i.or.kr/.19. Sasako M, Sano T, Yamamoto S, Sairenji M, Arai K, Kinoshita T, et al. Left thoracoabdominal approach versus abdominaltranshiatal approach for gastric cancer of the cardia or subcardia: a randomised controlled trial. Lancet Oncol. 2006; 7:644–651. PMID: 16887481.
Article20. Piso P, Werner U, Lang H, Mirena P, Klempnauer J. Proximal versus distal gastric carcinoma--what are the differences? Ann Surg Oncol. 2000; 7:520–525. PMID: 10947021.
Article21. Maeda H, Okabayashi T, Nishimori I, Sugimoto T, Namikawa T, Dabanaka K, et al. Clinicopathologic features of adenocarcinoma at the gastric cardia: is it different from distal cancer of the stomach? J Am Coll Surg. 2008; 206:306–310. PMID: 18222384.
Article22. McColl KE. Cancer of the gastric cardia. Best Pract Res Clin Gastroenterol. 2006; 20:687–696. PMID: 16997153.
Article23. Hamilton SR, Aaltonen LA, editors. . Pathology and Genetics of Tumours of the Digestive System. 2000. 1st ed. Lyon: IARCPress;p. 281–292.24. Ectors N, Driessen A, De Hertog G, Lerut T, Geboes K. Is adenocarcinoma of the esophagogastric junction or cardia different from Barrett adenocarcinoma? Arch Pathol Lab Med. 2005; 129:183–185. PMID: 15679417.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Clinicopathological Features of Borrmann Type IV Gastric Carcinomas
- Clinicopathological Features of Replication Error-positive Tumors in Single or Multiple Gastric Carcinomas
- Clinicopathological Features and Survival of Patients with Gastric Cancer with a Family History: a Large Analysis of 2,736 Patients with Gastric Cancer
- Clinicopathological and endoscopic features of Helicobacter pylori infection-negative gastric cancer in Japan: a retrospective study
- Changes of the Clinicopathological Characteristics and Survival Rates of Gastric Cancer with Gastrectomy: 1990s vs early 2000s
