J Gastric Cancer.
2011 Dec;11(4):225-229.
The Single Incision Laparoscopic Intragastric Wedge Resection of Gastric Submucosal Tumor
- Affiliations
-
- 1Department of Surgery, Chungnam National University School of Medicine, Daejeon, Korea. seungnoh@cnu.ac.kr
Abstract
- PURPOSE
Laparoscopic wedge resection of gastric submucosal tumor may be difficult in case of the endophytic mass or the mass located unreachable area such as cardia, and intragastric approach can be useful. We would present the experiences of the intragastric wedge resection.
MATERIALS AND METHODS
There were 7 patients diagnosed as gastric submucosal tumor and underwent the intragastric wedge resection at Surgery, Chungnam National University Hospital. We reviewed medical record.
RESULTS
There were 3 male and 4 female. Mean age was 65 years-old (57~73). Mean body mass index was 26.28 kg/m2 (21.28~35.30). Location of lesions was 4 cardia, 2 fundus and 1 midbody, respectively. Mean operation time was 83.6 minutes (70~105). All patients were healed without any complication. Mean postoperative hospital stay was 5.4 days (4~6). Mean size was 2.7 cm (2.3~3.8). Pathologic finding was 5 gastrointestinal stromal tumor and 2 leiomyoma.
CONCLUSIONS
The single incision intragastric wedge resection of gastric submucosal tumor is feasible and acceptable, especially in mass of gastric upper part.
Keyword
MeSH Terms
Figure
-
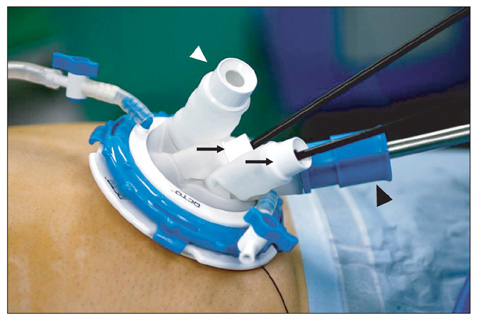
Fig. 1 Single port device (OCTO™ Dalim, Seoul, Korea) was placed at the umbilicus of patient. Th ere were 4 ports. A black arrow head (▴) is 5~12 mm transformable port. A white arrow head (▵) is 5/10 mm port with dual sealing mechanism. Two arrows (↑) are ports for 5 mm devices. In our procedure, the 5~12 mm port was for 10 mm telescope, 5/10 mm port was for 10 mm endo-GIA.
Reference
-
1. Kwon JG, Kim EY, Kim YS, Chun JW, Chung JT, You SS, et al. Accuracy of endoscopic ultrasonographic impression compared with pathologic diagnosis in gastrointestinal submucosal tumors. Korean J Gastroenterol. 2005. 45:88–96.2. Wiech T, Walch A, Werner M. Histopathological classification of nonneoplastic and neoplastic gastrointestinal submucosal lesions. Endoscopy. 2005. 37:630–634.
Article3. Casali PG, Jost L, Reichardt P, Schlemmer M, Blay JY. ESMO Guidelines Working Group. Gastrointestinal stromal tumours: ESMO clinical recommendations for diagnosis, treatment and follow-up. Ann Oncol. 2009. 20:Suppl 4. 64–67.
Article4. Ryu KJ, Jung SR, Choi JS, Jang YJ, Kim JH, Park SS, et al. Laparoscopic resection of small gastric submucosal tumors. Surg Endosc. 2011. 25:271–277.
Article5. Blackstein ME, Blay JY, Corless C, Driman DK, Riddell R, Soulières D, et al. Canadian Advisory Committee on GIST. Gastrointestinal stromal tumours: consensus statement on diagnosis and treatment. Can J Gastroenterol. 2006. 20:157–163.
Article6. Sasaki A, Koeda K, Obuchi T, Nakajima J, Nishizuka S, Terashima M, et al. Tailored laparoscopic resection for suspected gastric gastrointestinal stromal tumors. Surgery. 2010. 147:516–520.
Article7. Matthews BD, Walsh RM, Kercher KW, Sing RF, Pratt BL, Answini GA, et al. Laparoscopic vs open resection of gastric stromal tumors. Surg Endosc. 2002. 16:803–807.
Article8. Novitsky YW, Kercher KW, Sing RF, Heniford BT. Long-term outcomes of laparoscopic resection of gastric gastrointestinal stromal tumors. Ann Surg. 2006. 243:738–745.
Article9. Sexton JA, Pierce RA, Halpin VJ, Eagon JC, Hawkins WG, Linehan DC, et al. Laparoscopic gastric resection for gastrointestinal stromal tumors. Surg Endosc. 2008. 22:2583–2587.
Article10. Lai IR, Lee WJ, Yu SC. Minimally invasive surgery for gastric stromal cell tumors: intermediate follow-up results. J Gastrointest Surg. 2006. 10:563–566.
Article11. Tagaya N, Mikami H, Kogure H, Kubota K, Hosoya Y, Nagai H. Laparoscopic intragastric stapled resection of gastric submucosal tumors located near the esophagogastric junction. Surg Endosc. 2002. 16:177–179.
Article12. Li VK, Hung WK, Chung CK, Ying MW, Lam BY, Kan DM, et al. Laparoscopic intragastric approach for stromal tumours located at the posterior gastric wall. Asian J Surg. 2008. 31:6–10.
Article13. Uchikoshi F, Ito T, Nishida T, Kitagawa T, Endo S, Matsuda H. Laparoscopic intragastric resection of gastric stromal tumor located at the esophago-cardiac junction. Surg Laparosc Endosc Percutan Tech. 2004. 14:1–4.
Article14. Sekimoto M, Tamura S, Hasuike Y, Yano M, Murata A, Inoue M, et al. A new technique for laparoscopic resection of a submucosal tumor on the posterior wall of the gastric fundus. Surg Endosc. 1999. 13:71–74.
Article15. Shim JH, Lee HH, Yoo HM, Jeon HM, Park CH, Kim JG, et al. Intragastric approach for submucosal tumors located near the Z-line: a hybrid laparoscopic and endoscopic technique. J Surg Oncol. 2011. 104:312–315.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Single Port Laparoscopic Gastric Wedge Resection: Case Reports
- Choice of LECS Procedure for Benign and Malignant Gastric Tumors
- Laparoscopic Gastric Wedge Resection and Prophylactic Antireflux Surgery for a Submucosal Tumor of Gastroesophageal Junction
- Transumbilical Single-Incision Laparoscopic Wedge Resection for Gastric Submucosal Tumors: Technical Challenges Encountered in Initial Experience
- Single-incision intragastric resection for upper and mid gastric submucosal tumors: a case-series study
