J Korean Med Sci.
2017 Apr;32(4):650-655. 10.3346/jkms.2017.32.4.650.
Humidified High Flow Nasal Cannula versus Nasal Continuous Positive Airway Pressure as an Initial Respiratory Support in Preterm Infants with Respiratory Distress: a Randomized, Controlled Non-Inferiority Trial
- Affiliations
-
- 1Department of Pediatrics, Korea University College of Medicine, Seoul, Korea. cbmin@korea.ac.kr
- 2So Pediatric Clinic, Seoul, Korea.
- KMID: 2371451
- DOI: http://doi.org/10.3346/jkms.2017.32.4.650
Abstract
- Heated, humidified, high-flow nasal cannula (HHFNC) is frequently used as a noninvasive respiratory support for preterm infants with respiratory distress. But there are limited studies that compares HHFNC with nasal continuous positive airway pressure (nCPAP) only as the initial treatment of respiratory distress in preterm infants immediately after birth. The aim of this study is to assess the effectiveness and safety of HHFNC compared to nCPAP for the initial treatment of preterm infants with respiratory distress. Preterm infants at between 30 and 35 weeks of gestational age were randomized to HHFNC or nCPAP when they showed respiratory distress in less than 24 hours of age postnatally. Preterm infants who needed invasive respiratory supports were excluded. Primary outcome was the incidence of treatment failure (defined as need for the intubation or mechanical ventilation). Eighty-five infants were analyzed. Sixteen of 42 infants randomized to HHFNC showed treatment failure compared to 9 of 43 infants using nCPAP (Risk difference 17.17 [−1.90-36.23]; P = 0.099). In terms of the reason for treatment failure, the frequency of hypoxia was significantly higher in the HHFNC group than in the nCPAP group (P = 0.020). There was no difference between the 2 groups in terms of respiratory and clinical outcomes and complications. Although HHFNC is safe compared to nCPAP, it is not certain that HHFNC is effective compared to nCPAP non-inferiorly as an initial respiratory support in preterm infants with respiratory distress.
Keyword
Figure
-
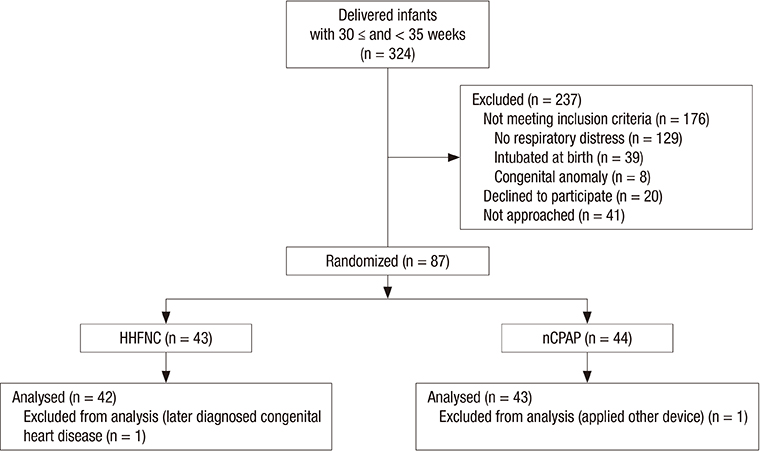
Fig. 1 Flowchart for describing enrollment. HHFNC = heated, humidified, high flow nasal cannula, nCPAP = nasal continuous positive airway pressure.
Reference
-
1. Schmölzer GM, Kumar M, Pichler G, Aziz K, O’Reilly M, Cheung PY. Non-invasive versus invasive respiratory support in preterm infants at birth: systematic review and meta-analysis. BMJ. 2013; 347:oct17 3. f5980.2. Dani C, Pratesi S, Migliori C, Bertini G. High flow nasal cannula therapy as respiratory support in the preterm infant. Pediatr Pulmonol. 2009; 44:629–634.3. Wilkinson D, Andersen C, O’Donnell CP, De Paoli AG, Manley BJ. High flow nasal cannula for respiratory support in preterm infants. Cochrane Database Syst Rev. 2016; 2:CD006405.4. Ciuffini F, Pietrasanta C, Lavizzari A, Musumeci S, Gualdi C, Sortino S, Colnaghi M, Mosca F. Comparison between two different modes of non-invasive ventilatory support in preterm newborn infants with respiratory distress syndrome mild to moderate: preliminary data. Pediatr Med Chir. 2014; 36:88.5. Iranpour R, Sadeghnia A, Abari SS. High flow nasal cannula in the treatment of respiratory distress syndrome in one day-old neonate. Br J Med Med Res. 2016; 15:1–7.6. Jobe AH, Bancalari E. Bronchopulmonary dysplasia. Am J Respir Crit Care Med. 2001; 163:1723–1729.7. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978; 92:529–534.8. de Vries LS, Eken P, Dubowitz LM. The spectrum of leukomalacia using cranial ultrasound. Behav Brain Res. 1992; 49:1–6.9. Kliegman RM, Walsh MC. Neonatal necrotizing enterocolitis: pathogenesis, classification, and spectrum of illness. Curr Probl Pediatr. 1987; 17:213–288.10. Manley BJ, Owen LS, Doyle LW, Andersen CC, Cartwright DW, Pritchard MA, Donath SM, Davis PG. High-flow nasal cannulae in very preterm infants after extubation. N Engl J Med. 2013; 369:1425–1433.11. Piaggio G, Elbourne DR, Pocock SJ, Evans SJ, Altman DG, CONSORT Group ; CONSORT Group. Reporting of noninferiority and equivalence randomized trials: extension of the CONSORT 2010 statement. JAMA. 2012; 308:2594–2604.12. Yoder BA, Stoddard RA, Li M, King J, Dirnberger DR, Abbasi S. Heated, humidified high-flow nasal cannula versus nasal CPAP for respiratory support in neonates. Pediatrics. 2013; 131:e1482–90.13. Lavizzari A, Veneroni C, Colnaghi M, Ciuffini F, Zannin E, Fumagalli M, Mosca F, Dellacà RL. Respiratory mechanics during NCPAP and HHHFNC at equal distending pressures. Arch Dis Child Fetal Neonatal Ed. 2014; 99:F315–20.14. Dysart K, Miller TL, Wolfson MR, Shaffer TH. Research in high flow therapy: mechanisms of action. Respir Med. 2009; 103:1400–1405.15. Kubicka ZJ, Limauro J, Darnall RA. Heated, humidified high-flow nasal cannula therapy: yet another way to deliver continuous positive airway pressure? Pediatrics. 2008; 121:82–88.16. Locke RG, Wolfson MR, Shaffer TH, Rubenstein SD, Greenspan JS. Inadvertent administration of positive end-distending pressure during nasal cannula flow. Pediatrics. 1993; 91:135–138.17. Sivieri EM, Gerdes JS, Abbasi S. Effect of HFNC flow rate, cannula size, and nares diameter on generated airway pressures: an in vitro study. Pediatr Pulmonol. 2013; 48:506–514.18. Collins CL, Holberton JR, Barfield C, Davis PG. A randomized controlled trial to compare heated humidified high-flow nasal cannulae with nasal continuous positive airway pressure postextubation in premature infants. J Pediatr. 2013; 162:945–954 e1.19. Collins CL, Barfield C, Horne RS, Davis PG. A comparison of nasal trauma in preterm infants extubated to either heated humidified high-flow nasal cannulae or nasal continuous positive airway pressure. Eur J Pediatr. 2014; 173:181–186.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Respiratory support with heated humidified high flow nasal cannula in preterm infants
- High-flow nasal cannula oxygen therapy in children: a clinical review
- High Flow Nasal Cannula versus Nasal CPAP in Preterm Infants
- Comparison of Effectiveness of Nasal Continuous Positive Airway Pressure and Nasal Intermittent Positive Pressure Ventilation for the Initial Treatment of Preterm Respiratory Distress Syndrome: A Prospective Pilot Study
- Modified high-flow nasal cannula for children with respiratory distress
