Massive pericardial effusion and short stature caused by autoimmune hypothyroidism in a 9-year-old girl
- Affiliations
-
- 1Department of Pediatrics, Chungbuk National University College of Medicine, Cheongju, Korea. hshan@chungbuk.ac.kr
- KMID: 2368993
- DOI: http://doi.org/10.6065/apem.2015.20.2.98
Abstract
- A 9-year-, 11-month-old girl was brought to the Emergency Department for sudden dyspnea caused by massive pericardial effusion. In addition to relative bradycardia despite impending cardiac tamponade, short stature, overweight, and hypercholesterolemia were clues for suspected hypothyroidism. During thyroxine supplementation, catch-up growth was incomplete by rapid skeletal maturation. The use of short-term growth hormone showed increased growth velocity. In conclusion, primary hypothyroidism should be included in the etiologic evaluation of pericardial effusion, especially when it is associated with relative bradycardia. Additional growth promoting therapy should be considered for incomplete catch-up growth in prolonged hypothyroidism during thyroxine supplementation.
MeSH Terms
Figure
-

Fig. 1 Echocardiography revealed massive pericardial effusion around the heart and fluctuating mitral inflow pattern recorded according to respiration (A), and closed pericardiostomy was performed with pericardial catheter (B).
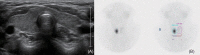
Fig. 2 Thyroid ultrasonography showed mild heterogeneous echogenicity without intrathyroid nodule and lymph node enlargement (A), and thyroid 99mTc scintigram showed focal increase of radio-uptake in right lobe and nearly non-visualization of left lobe (B).

Fig. 3 Height standard deviation score (HSDS) improved during 1st year of thyroxine (T4) replacement with appropriate bone age (BA) progression. But during next 6 months, BA progressed rapidly without improvement of HSDS. Growth hormone was tried for the next 6 months with remarkable increase of HSDS. BMI, body mass index; CA, chronologic age.
Cited by 1 articles
-
Diagnostic difficulties by the unusual presentations in children and adolescents with Hashimoto thyroiditis
Betül Ersoy, Kiremitçi Yılmaz Seniha, Deniz Kızılay, Münevver Yılmaz, Şenol Coşkun
Ann Pediatr Endocrinol Metab. 2016;21(3):164-168. doi: 10.6065/apem.2016.21.3.164.
Reference
-
1. Rosenfeld RG, Cohen P. Disorders of growth hormone/insulin-like growth factor secretion and action. In : Sperling MA, editor. Pediatric endocrinology. 3rd ed. Philadelphia: Saunders Elsevier;2008. p. 287–288.2. Korean society of pediatric endocrinology. Pediatric endocrinology. 3rd ed. Seoul: Koonja;2014. p. 205–209.3. Williams LH, Jayatunga R, Scott O. Massive pericardial effusion in a hypothyroid child. Br Heart J. 1984; 51:231–232. PMID: 6229261.
Article4. Rivkees SA, Bode HH, Crawford JD. Long-term growth in juvenile acquired hypothyroidism: the failure to achieve normal adult stature. N Engl J Med. 1988; 318:599–602. PMID: 3344006.
Article5. Larson NS, Pinsker JE. Primary hypothyroidism with growth failure and pituitary pseudotumor in a 13-year-old female: a case report. J Med Case Rep. 2013; 7:149. PMID: 23725039.
Article6. Kang SY, Park WS, Jung MJ, Lee YS, Park SG, Yu J. Two cases of acquired hypothyroidism with severe obesity, short stature and cardiomegaly. J Korean Soc Pediatr Endocrinol. 2003; 8:189–195.7. Chen YJ, Hou SK, How CK, Chern CH, Lo HC, Yen DH, et al. Diagnosis of unrecognized primary overt hypothyroidism in the ED. Am J Emerg Med. 2010; 28:866–870. PMID: 20887907.
Article8. Ekka M, Ali I, Aggarwal P, Jamshed N. Cardiac tamponade as initial presenting feature of primary hypothyroidism in the ED. Am J Emerg Med. 2014; 32:683.e1–683.e3. PMID: 24360319.
Article9. Setty NS, Sadananda KS, Nanjappa MC, Patra S, Basappa H, Krishnappa S. Massive pericardial effusion and cardiac tamponade due to cholesterol pericarditis in a case of subclinical hypothyroidism: a rare event. J Am Coll Cardiol. 2014; 63:1451. PMID: 24561150.
Article10. Shastry RM, Shastry CC. Primary hypothyroidism with pericardial tamponade. Indian J Pediatr. 2007; 74:580–581. PMID: 17595503.
Article11. Sanda S, Newfield RS. A child with pericardial effusion and cardiac tamponade due to previously unrecognized hypothyroidism. J Natl Med Assoc. 2007; 99:1411–1413. PMID: 18229779.12. Mokta J, Mokta K, Panda P, Sharma M, Bhatia V. A swinging heart. Indian J Endocrinol Metab. 2013; 17(Suppl 3):S660–S661. PMID: 24910831.
Article13. Purkait R, Prasad A, Bhadra R, Basu A. Massive pericardial effusion as the only manifestation of primary hypothyroidism. J Cardiovasc Dis Res. 2013; 4:248–250. PMID: 24653591.
Article14. Nanto-Salonen K, Muller HL, Hoffman AR, Vu TH, Rosenfeld RG. Mechanisms of thyroid hormone action on the insulin-like growth factor system: all thyroid hormone effects are not growth hormone mediated. Endocrinology. 1993; 132:781–788. PMID: 7678799.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Primary HypoThyroidism Presenting with Pericardial Effusion
- A case of pregnancy complicated primary hypothyroidism presenting with cardiac tamonade resulted from massive pericardial effusion and megacolon
- A Case of Autoimmune Hemolytic Anemia & Pericardial Effusion Developed in Hashimoto's Thyroiditis Patient
- A Case of Behcet's Syndrome with Superior Vena Cava Obstruction and Massive Pericardial Effusion
- Two Cases of Acquired Hypothyroidism with Severe Obesity, Short Stature and Cardiomegaly
