Could Psoriatic Arthritis Be Easily Diagnosed from Current Suspicious Physical Findings in the Dermatology Clinic?
- Affiliations
-
- 1Department of Dermatology, Seoul National University Bundang Hospital, Seoul National University College of Medicine, Seongnam, Korea. swyoun@snu.ac.kr
- KMID: 2368027
- DOI: http://doi.org/10.5021/ad.2017.29.1.48
Abstract
- BACKGROUND
The prevalence and clinical characteristics of psoriatic arthritis (PsA) in patients with psoriasis are not well described in Asian populations, including Koreans.
OBJECTIVE
The purpose of this study was to investigate the prevalence of PsA by using the classification of psoriatic arthritis (CASPAR) criteria on the basis of physical examination only, as well as its correlation with psoriasis severity and other medical conditions including nail psoriasis.
METHODS
A single-center, cross-sectional observational cohort study was conducted, and the included patients were evaluated for PsA according to the CASPAR criteria. The psoriasis area severity index (PASI) and the nail psoriasis severity index (NAPSI) were calculated.
RESULTS
The prevalence of PsA in patients with psoriasis in Korea was 13.5%. When performing logistic regression, hyperlipidemia and localized pustular psoriasis were found to be significant predictors of PsA. The PASI score was significantly higher in PsA patients than in those with psoriasis alone (p=0.014). Psoriatic nail involvement was found in 85.5% of the study population, and all PsA patients had nail psoriasis. The mean NAPSI score was higher in patients with PsA; however, the difference was not statistically significant.
CONCLUSION
There was a close relation between psoriasis severity and PsA, although nail psoriasis severity was not related to PsA status. Dermatologists can diagnose PsA from current physical findings by using the CASPAR criteria. To validate the CASPAR criteria for PsA diagnosis, the definition of nail psoriasis clinical types and severity in the CASPAR criteria should be reviewed again.
Keyword
MeSH Terms
Figure
-
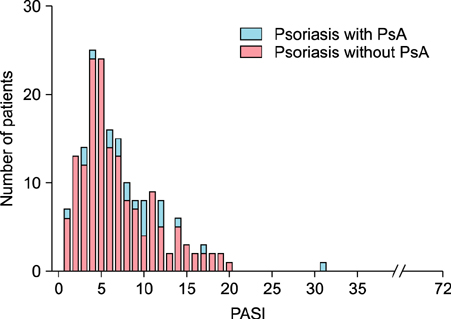
Fig. 1 Frequency distributions of patients in psoriasis area severity index (PASI) values according to psoriatic arthritis (PsA) status.
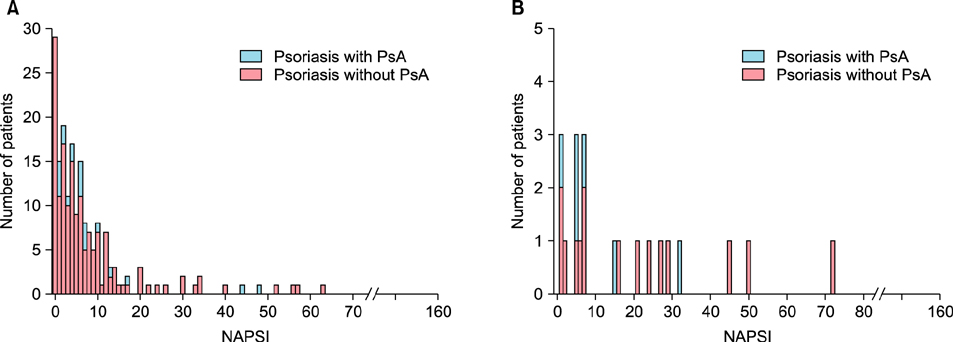
Fig. 2 The frequency distribution of patient in nail psoriasis severity index (NAPSI) values according to presence or absence of psoriatic arthritis (PsA) for the two different types of psoriasis, plaque psoriasis (A) and localized pustular psoriasis (B).
Cited by 2 articles
-
Recent medical therapy for psoriasis
Sang Woong Youn
J Korean Med Assoc. 2019;62(3):176-180. doi: 10.5124/jkma.2019.62.3.176.Clinical Characteristics of Patients With Psoriatic Spondylitis Versus Those With Ankylosing Spondylitis: Features at Baseline Before Biologic Therapy
Hyoun-Ah Kim, Eunyoung Lee, So Young Park, Shin-Seok Lee, Kichul Shin
J Korean Med Sci. 2022;37(33):e253. doi: 10.3346/jkms.2022.37.e253.
Reference
-
1. Youn SW, Kim BR, Lee JH, Song HJ, Choe YB, Choi JH, et al. Comparison of treatment goals for moderate-to-severe psoriasis between Korean dermatologists and the European consensus report. Ann Dermatol. 2015; 27:184–189.
Article2. Prey S, Paul C, Bronsard V, Puzenat E, Gourraud PA, Aractingi S, et al. Assessment of risk of psoriatic arthritis in patients with plaque psoriasis: a systematic review of the literature. J Eur Acad Dermatol Venereol. 2010; 24:Suppl 2. 31–35.
Article3. Schön MP, Boehncke WH. Psoriasis. N Engl J Med. 2005; 352:1899–1912.
Article4. Ciocon DH, Kimball AB. Psoriasis and psoriatic arthritis: separate or one and the same? Br J Dermatol. 2007; 157:850–860.
Article5. Ackermann C, Kavanaugh A. Economic burden of psoriatic arthritis. Pharmacoeconomics. 2008; 26:121–129.
Article6. Feldman SR, Zhao Y, Shi L, Tran MH, Lu J. Economic and comorbidity burden among moderate-to-severe psoriasis patients with comorbid psoriatic arthritis. Arthritis Care Res (Hoboken). 2015; 67:708–717.
Article7. McHugh NJ, Balachrishnan C, Jones SM. Progression of peripheral joint disease in psoriatic arthritis: a 5-yr prospective study. Rheumatology (Oxford). 2003; 42:778–783.
Article8. Callis Duffin K, Wong B, Horn EJ, Krueger GG. Psoriatic arthritis is a strong predictor of sleep interference in patients with psoriasis. J Am Acad Dermatol. 2009; 60:604–608.
Article9. Brockbank J, Gladman D. Diagnosis and management of psoriatic arthritis. Drugs. 2002; 62:2447–2457.
Article10. Haroon M, Kirby B, FitzGerald O. High prevalence of psoriatic arthritis in patients with severe psoriasis with suboptimal performance of screening questionnaires. Ann Rheum Dis. 2013; 72:736–740.
Article11. Taylor W, Gladman D, Helliwell P, Marchesoni A, Mease P, Mielants H. CASPAR Study Group. Classification criteria for psoriatic arthritis: development of new criteria from a large international study. Arthritis Rheum. 2006; 54:2665–2673.
Article12. Englbrecht M, Wang Y, Ronneberger M, Manger B, Vastesaeger N, Veale DJ, et al. Measuring joint involvement in polyarticular psoriatic arthritis: an introduction of alternatives. Arthritis Care Res (Hoboken). 2010; 62:977–983.
Article13. Rich P, Scher RK. Nail psoriasis severity index: a useful tool for evaluation of nail psoriasis. J Am Acad Dermatol. 2003; 49:206–212.
Article14. Ibrahim GH, Buch MH, Lawson C, Waxman R, Helliwell PS. Evaluation of an existing screening tool for psoriatic arthritis in people with psoriasis and the development of a new instrument: the Psoriasis Epidemiology Screening Tool (PEST) questionnaire. Clin Exp Rheumatol. 2009; 27:469–474.15. Moll JM, Wright V. Psoriatic arthritis. Semin Arthritis Rheum. 1973; 3:55–78.
Article16. Yang Q, Qu L, Tian H, Hu Y, Peng J, Yu X, et al. Prevalence and characteristics of psoriatic arthritis in Chinese patients with psoriasis. J Eur Acad Dermatol Venereol. 2011; 25:1409–1414.
Article17. Kawada A, Tezuka T, Nakamizo Y, Kimura H, Nakagawa H, Ohkido M, et al. A survey of psoriasis patients in Japan from 1982 to 2001. J Dermatol Sci. 2003; 31:59–64.
Article18. Ohara Y, Kishimoto M, Takizawa N, Yoshida K, Okada M, Eto H, et al. Prevalence and clinical characteristics of psoriatic arthritis in Japan. J Rheumatol. 2015; 42:1439–1442.
Article19. Fan X, Yang S, Sun LD, Liang YH, Gao M, Zhang KY, et al. Comparison of clinical features of HLA-Cw*0602-positive and -negative psoriasis patients in a Han Chinese population. Acta Derm Venereol. 2007; 87:335–340.
Article20. Wu S, Li WQ, Han J, Sun Q, Qureshi AA. Hypercholesterolemia and risk of incident psoriasis and psoriatic arthritis in US women. Arthritis Rheumatol. 2014; 66:304–310.
Article21. Baek HJ, Yoo CD, Shin KC, Lee YJ, Kang SW, Lee EB, et al. Spondylitis is the most common pattern of psoriatic arthritis in Korea. Rheumatol Int. 2000; 19:89–94.
Article22. Rouzaud M, Sevrain M, Villani AP, Barnetche T, Paul C, Richard MA, et al. Is there a psoriasis skin phenotype associated with psoriatic arthritis? Systematic literature review. J Eur Acad Dermatol Venereol. 2014; 28:Suppl 5. 17–26.
Article23. Farber EM, Nall L. Nail psoriasis. Cutis. 1992; 50:174–178.24. Augustin M, Reich K, Blome C, Schäfer I, Laass A, Radtke MA. Nail psoriasis in Germany: epidemiology and burden of disease. Br J Dermatol. 2010; 163:580–585.
Article25. Mease PJ, Gladman DD, Papp KA, Khraishi MM, Thaçi D, Behrens F, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013; 69:729–735.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Psoriatic Arthritis
- Mutilating Psoriatic Arthritis: A case report
- A Case of Nail Psoriasis Improved by Treatment with Golimumab in a Psoriatic Arthritis Patient
- Association Between Psoriasis and HLA - B27 Antigen
- Screening for Psoriatic Arthritis in Korean Psoriasis Patients Using the Psoriatic Arthritis Screening Evaluation Questionnaire
