Short stature and growth hormone deficiency in a girl with encephalocraniocutaneous lipomatosis and Jaffe-Campanacci syndrome: a case report
- Affiliations
-
- 1Department of Pediatrics, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea. kimhs@dsmc.or.kr
- 2Department of Orthopedics, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea.
- 3Department of Radiology, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea.
- 4Department of Pathology, Keimyung University Dongsan Medical Center, Keimyung University School of Medicine, Daegu, Korea.
- KMID: 2366817
- DOI: http://doi.org/10.6065/apem.2016.21.4.240
Abstract
- A 9-year-old Tajikistani girl presented to Keimyung University Dongsan Medical Center for evaluation of a skin lesion on her left eyelid, focal alopecia, unilateral ventricular dilatation, and aortic coarctation. She was diagnosed with encephalocraniocutaneous lipomatosis (ECCL) according to Moog's diagnostic criteria. Café-au-lait spots were found on the left side of her trunk. Multiple nonossifying fibromas were found on her left proximal humerus, left distal femur, both proximal tibias, and left proximal fibula, suggesting Jaffe-Campanacci syndrome (JCS), following imaging of the extremities. Many JCS cases with multiple Café-au-lait macules, multiple nonossifying fibromas may actually have Neurofibromatosis type-1 (NF1). Thus, comprehensive molecular analysis to exclude NF1 mutation was performed using her blood sample. The NF1 mutation was not found. Her height was under the 3rd percentile and her bone age was delayed as compared with her chronological age. Baseline growth hormone (GH) level was below the normal range. Using the insulin stimulation and levo-dihydroxyphenylalanine tests, GH deficiency was confirmed. We present a case of GH deficiency with typical features of ECCL and JCS.
Figure
-

Fig. 1 Morphologic characteristics of a girl with encephalocraniocutaneous lipomatosis and Jaffe-Campanacci syndrome. (A) A view of the whole body. (B) In the left upper eyelid, coloboma and cryptophthalmos with dermolipoma are shown. In the medial half of the upper eyelid, an irregular lid margin and cilial defects are shown. There was an approximately 1 cm-sized round movable nontender mass on her medial upper eyelid. In the conjunctiva, an approximately 5 mm in diameter round hyperemic cyst-like lesion was located on the nasal side. Diffuse conjunctivalization of the cornea and engorged vessels on the nasal side were also observed. (C) Congenital absence or deficiency of a localized area of skin, with the base of the defect covered by a thin translucent membrane is shown. (D) Possible nevus psiloliparus (skin biopsy was not performed) is shown. (E) Hyperpigmentation with a café-au-lait macule is shown. (F) Hemihypertrophy of the left lower limb is shown.
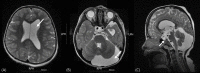
Fig. 2 Magnetic resonance imaging of the brain in a girl with encephalocraniocutaneous lipomatosis. (A) Unilateral ventricular dilatation can be seen (arrow). (B) An extra-axial cerebrospinal fluid space in the left hemisphere and posterior fossa are visible (arrow). (C) The sella turcica was intact on the sagittal view (arrow).
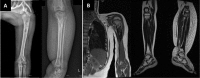
Fig. 3 Images of a girl with encephalocraniocutaneous lipomatosis and Jaffe-Campanacci syndrome. (A) Humerus X-ray shows nonossifying fibromas involving the left proximal humerus and left tibiae. (B) Magnetic resonance imaging shows a relatively welldefined, elongated cortical bone lesion involving the left proximal humerus with heterogeneous enhancement suggestive of nonossifyping fibromata extraskeletal anomalies, or angiomatosis, and lipomatosis involving the left tibiae, which can be found in the Jaffe Campanacci syndrome.
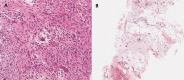
Fig. 4 Histopathologic findings in a girl with encephalocraniocutaneous lipomatosis and Jaffe-Campanacci syndrome. (A) Tibia bone biopsy suggestive of metaphyseal fibrous defect, focal fatty-vascular tissue proliferation, and non-ossifying fibroma (H&E, ×200). (B) Pretibial soft tissue biopsy suggestive of lipomatosis and fatty tissue proliferation (H&E, ×100).
Reference
-
1. Banta J, Beasley K, Kobayashi T, Rohena L. Encephalocraniocutaneous lipomatosis (Haberland syndrome): a mild case with bilateral cutaneous and ocular involvement. JAAD Case Rep. 2016; 2:150–152. PMID: 27222873.
Article2. Chandravanshi SL. Encephalocraniocutaneous lipomatosis: a case report and review of the literature. Indian J Ophthalmol. 2014; 62:622–627. PMID: 24881613.
Article3. Sharifi M, Namdari M. Encephalocraniocutaneous lipomatosis (Fishman syndrome): a rare neurocutaneous syndrome. J Curr Ophthalmol. 2016; 28:155–158. PMID: 27579462.
Article4. Cherix S, Bildé Y, Becce F, Letovanec I, Rüdiger HA. Multiple non-ossifying fibromas as a cause of pathological femoral fracture in Jaffe-Campanacci syndrome. BMC Musculoskelet Disord. 2014; 15:218. PMID: 24965055.
Article5. Hau MA, Fox EJ, Cates JM, Brigman BE, Mankin HJ. Jaffe-Campanacci syndrome. A case report and review of the literature. J Bone Joint Surg Am. 2002; 84-A:634–638. PMID: 11940628.6. Moog U. Encephalocraniocutaneous lipomatosis. J Med Genet. 2009; 46:721–729. PMID: 19574261.
Article7. Radić Nišević J, Prpić I, Antulov R, Sasso A, Holjar Erlić I. Encephalocraniocutaneous lipomatosis without ocular malformations. Pediatr Neurol. 2016; 60:71–74. PMID: 27131628.8. Ahmed I, Tope WD, Young TL, Miller DM, Bloom KE. Neurocutaneous melanosis in association with encephalocraniocutaneous lipomatosis. J Am Acad Dermatol. 2002; 47(2 Suppl):S196–S200. PMID: 12140461.
Article9. Gokhale NR, Mahajan PM, Belgaumkar VA, Pradhan SN, Uttarwar NS. Encephalocraniocutaneous lipomatosis: a rare neurocutaneous syndrome. Indian J Dermatol Venereol Leprol. 2007; 73:40–42. PMID: 17314447.
Article10. Campanacci M, Laus M, Boriani S. Multiple non-ossifying fibromata with extraskeletal anomalies: a new syndrome. J Bone Joint Surg Br. 1983; 65:627–632. PMID: 6643569.
Article11. Stewart DR, Brems H, Gomes AG, Ruppert SL, Callens T, Williams J, et al. Jaffe-Campanacci syndrome, revisited: detailed clinical and molecular analyses determine whether patients have neurofibromatosis type 1, coincidental manifestations, or a distinct disorder. Genet Med. 2014; 16:448–459. PMID: 24232412.
Article
