Robotic Low Ligation of the Inferior Mesenteric Artery for Rectal Cancer Using the Firefly Technique
- Affiliations
-
- 1Division of Colorectal Surgery, Department of Surgery, School of Medicine, Keimyung University and Dongsan Medical Center, Daegu, Korea.
- 2Division of Colorectal Surgery, Department of Surgery, Colorectal Cancer Clinic, Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. namkyuk@yuhs.ac
- KMID: 2366345
- DOI: http://doi.org/10.3349/ymj.2015.56.4.1028
Abstract
- PURPOSE
By integrating intraoperative near infrared fluorescence imaging into a robotic system, surgeons can identify the vascular anatomy in real-time with the technical advantages of robotics that is useful for meticulous lymphovascular dissection. Herein, we report our initial experience of robotic low ligation of the inferior mesenteric artery (IMA) with real-time identification of the vascular system for rectal cancer using the Firefly technique.
MATERIALS AND METHODS
The study group included 11 patients who underwent a robotic total mesorectal excision with preservation of the left colic artery for rectal cancer using the Firefly technique between July 2013 and December 2013.
RESULTS
The procedures included five low anterior resections and six ultra-low anterior resections with loop ileostomy. The median total operation time was 327 min (226-490). The low ligation time was 10 min (6-20), and the time interval between indocyanine green injection and division of the sigmoid artery was 5 min (2-8). The estimated blood loss was 200 mL (100-500). The median time to soft diet was 4 days (4-5), and the median length of stay was 7 days (5-9). Three patients developed postoperative complications; one patients developed anal stricture, one developed ileus, and one developed non-complicated intraabdominal fluid collection. The median total number of lymph nodes harvested was 17 (9-29).
CONCLUSION
Robotic low ligation of the IMA with real-time identification of the vascular system for rectal cancer using the Firefly technique is safe and feasible. This technique can allow for precise lymph node dissection along the IMA and facilitate the identification of the left colic branch of the IMA.
MeSH Terms
-
Aged
Aged, 80 and over
Digestive System Surgical Procedures/methods
Female
Humans
Ligation/methods
Lymph Node Excision/*methods
Lymph Nodes/pathology/surgery
Male
*Mesenteric Artery, Inferior
Middle Aged
Minimally Invasive Surgical Procedures/methods
Postoperative Complications/surgery
Rectal Neoplasms/pathology/*surgery
Rectum/*surgery
Robotics/*methods
Time Factors
Treatment Outcome
Figure
-
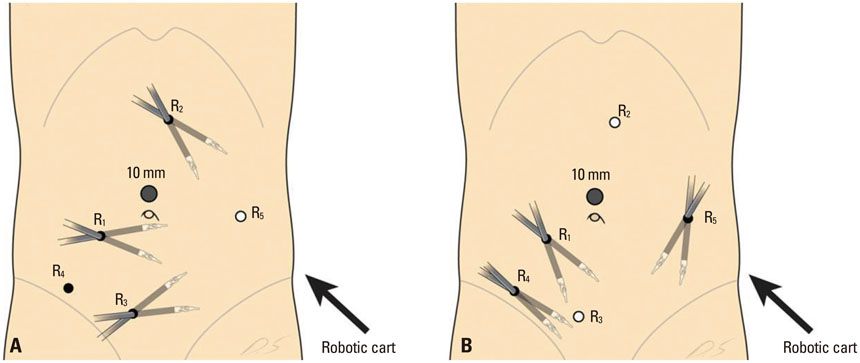
Fig. 1 Port placement for totally robotic rectal surgery using the single docking dual phase technique. (A) Port placement in the colonic stage. (B) Port placement in the pelvic stage.
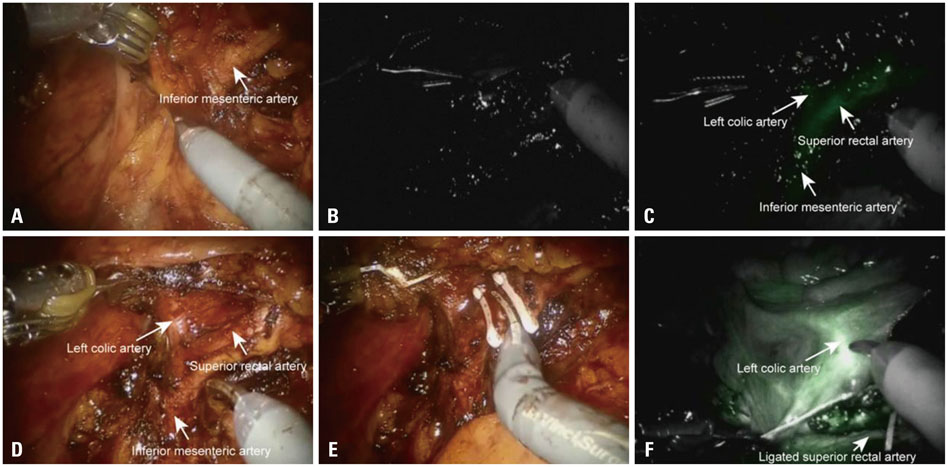
Fig. 2 Robotic-assisted lymph node dissection around the IMA with preservation of the LCA using the Firefly technique. (A) Dissection around the root of the IMA (white light image). (B) INIF image before visualizing the LCA by excited fluorescence. (C) INIF image of visualizing the LCA by excited fluorescence. (D)Skeletonization of the LCA and SRA from the IMA. (E) Low ligation of the IMA preserving the left colic branch. (F) Confirmation of blood flow of the LCA by INIF imaging. IMA, inferior mesenteric artery; LCA, left colic artery; INIF, intraoperative near infrared fluorescence; SRA, superior rectal artery.
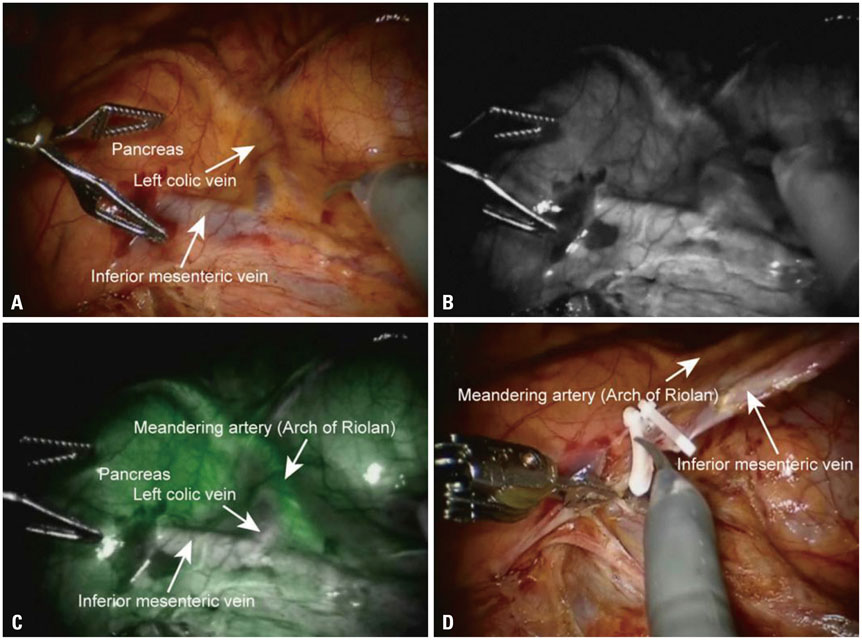
Fig. 3 Identification of the collateral artery near the IMV and pancreas. (A) Assessing the anatomical blood supply around the pancreas and IMV (white light image). (B) INIF imaging before visualizing the vascular flow by excited fluorescence. (C) INIF image of visualized arterial flow by excited fluorescence. (D)High ligation of the IMV with avoidance of injury to collateral vessels. IMV, inferior mesenteric vein; INIF, intraoperative near infrared fluorescence.
Cited by 3 articles
-
Operative safety and oncologic outcomes in rectal cancer based on the level of inferior mesenteric artery ligation: a stratified analysis of a large Korean cohort
Mohammed A. AlSuhaimi, Seung Yoon Yang, Jae Hyun Kang, Jamal F. AlSabilah, Hyuk Hur, Nam Kyu Kim
Ann Surg Treat Res. 2019;97(5):254-260. doi: 10.4174/astr.2019.97.5.254.Robotic surgery for colorectal disease: review of current port placement and future perspectives
Jong Lyul Lee, Hassan A. Alsaleem, Jin Cheon Kim
Ann Surg Treat Res. 2020;98(1):31-43. doi: 10.4174/astr.2020.98.1.31.Robotic Surgery for Rectal Cancer: An Update in 2015
Jung Myun Kwak, Seon Hahn Kim
Cancer Res Treat. 2016;48(2):427-435. doi: 10.4143/crt.2015.478.
Reference
-
1. Kingham TP, Pachter HL. Colonic anastomotic leak: risk factors, diagnosis, and treatment. J Am Coll Surg. 2009; 208:269–278.
Article2. McArdle CS, McMillan DC, Hole DJ. Impact of anastomotic leakage on long-term survival of patients undergoing curative resection for colorectal cancer. Br J Surg. 2005; 92:1150–1154.
Article3. Park YA, Kim JM, Kim SA, Min BS, Kim NK, Sohn SK, et al. Totally robotic surgery for rectal cancer: from splenic flexure to pelvic floor in one setup. Surg Endosc. 2010; 24:715–720.
Article4. Chapuis PH, Dent OF, Fisher R, Newland RC, Pheils MT, Smyth E, et al. A multivariate analysis of clinical and pathological variables in prognosis after resection of large bowel cancer. Br J Surg. 1985; 72:698–702.
Article5. Lindmark G, Gerdin B, Påhlman L, Bergström R, Glimelius B. Prognostic predictors in colorectal cancer. Dis Colon Rectum. 1994; 37:1219–1227.
Article6. Kanemitsu Y, Hirai T, Komori K, Kato T. Survival benefit of high ligation of the inferior mesenteric artery in sigmoid colon or rectal cancer surgery. Br J Surg. 2006; 93:609–615.
Article7. Chin CC, Yeh CY, Tang R, Changchien CR, Huang WS, Wang JY. The oncologic benefit of high ligation of the inferior mesenteric artery in the surgical treatment of rectal or sigmoid colon cancer. Int J Colorectal Dis. 2008; 23:783–788.
Article8. Kang J, Hur H, Min BS, Kim NK, Lee KY. Prognostic impact of inferior mesenteric artery lymph node metastasis in colorectal cancer. Ann Surg Oncol. 2011; 18:704–710.
Article9. Komen N, Slieker J, de Kort P, de Wilt JH, van der Harst E, Coene PP, et al. High tie versus low tie in rectal surgery: comparison of anastomotic perfusion. Int J Colorectal Dis. 2011; 26:1075–1078.
Article10. Hellan M, Spinoglio G, Pigazzi A, Lagares-Garcia JA. The influence of fluorescence imaging on the location of bowel transection during robotic left-sided colorectal surgery. Surg Endosc. 2014; 28:1695–1702.
Article11. Höer J, Roegels A, Prescher A, Klosterhalfen B, Töns C, Schum-pelick V. [Preserving autonomic nerves in rectal surgery. Results of surgical preparation on human cadavers with fixed pelvic sections]. Chirurg. 2000; 71:1222–1229.
Article12. Nano M, Dal Corso H, Ferronato M, Solej M, Hornung JP, Dei Poli M. Ligation of the inferior mesenteric artery in the surgery of rectal cancer: anatomical considerations. Dig Surg. 2004; 21:123–126.
Article13. Hinoi T, Okajima M, Shimomura M, Egi H, Ohdan H, Konishi F, et al. Effect of left colonic artery preservation on anastomotic leakage in laparoscopic anterior resection for middle and low rectal cancer. World J Surg. 2013; 37:2935–2943.
Article14. Kobayashi M, Okamoto K, Namikawa T, Okabayashi T, Araki K. Laparoscopic lymph node dissection around the inferior mesenteric artery for cancer in the lower sigmoid colon and rectum: is D3 lymph node dissection with preservation of the left colic artery feasible? Surg Endosc. 2006; 20:563–569.
Article15. Krane LS, Manny TB, Hemal AK. Is near infrared fluorescence imaging using indocyanine green dye useful in robotic partial nephrectomy: a prospective comparative study of 94 patients. Urology. 2012; 80:110–116.
Article16. Spinoglio G, Priora F, Bianchi PP, Lucido FS, Licciardello A, Maglione V, et al. Real-time near-infrared (NIR) fluorescent cholangiography in single-site robotic cholecystectomy (SSRC): a single-institutional prospective study. Surg Endosc. 2013; 27:2156–2162.
Article17. Miyashiro I, Miyoshi N, Hiratsuka M, Kishi K, Yamada T, Ohue M, et al. Detection of sentinel node in gastric cancer surgery by indocyanine green fluorescence imaging: comparison with infrared imaging. Ann Surg Oncol. 2008; 15:1640–1643.
Article18. Liang JT, Lai HS. Surgical technique of robotic D3 lymph node dissection around the inferior mesenteric artery with preservation of the left colic artery and autonomic nerves for the treatment of distal rectal cancer. Surg Endosc. 2014; 28:1727–1733.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Operative safety and oncologic outcomes in rectal cancer based on the level of inferior mesenteric artery ligation: a stratified analysis of a large Korean cohort
- Feasibility and oncologic safety of low ligation of inferior mesenteric artery with D3 dissection in cT3N0M0 sigmoid colon cancer
- Oncologic and Anastomotic Safety of Low Ligation of the Inferior Mesenteric Artery With Additional Lymph Node Retrieval: A Case-Control Study
- A Case of the Inferior Mesenteric Artery Arising from the Superior Mesenteric Artery in a Korean Woman
- Inferior Mesenteric Artery Embolization with N-Butyl Cyanoacrylate for Life-Threatening Postpartum Hemorrhage: A Report of Two Cases and Literature Review
