Yonsei Med J.
2015 Jul;56(4):998-1006. 10.3349/ymj.2015.56.4.998.
Prevention of Cytomegalovirus Transmission via Breast Milk in Extremely Low Birth Weight Infants
- Affiliations
-
- 1Department of Pediatrics, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. wonspark@skku.edu
- 2Department of Pediatrics, Haeundae Paik Hospital, Inje University School of Medicine, Busan, Korea.
- KMID: 2366341
- DOI: http://doi.org/10.3349/ymj.2015.56.4.998
Abstract
- PURPOSE
Extremely low birth weight infants (ELBWIs) have a high risk of acquiring cytomegalovirus (CMV) infection via breast milk and consequently developing serious symptoms. We evaluated whether freeze-thawing or pasteurization could prevent postnatal CMV infection transmitted through breast milk in ELBWIs.
MATERIALS AND METHODS
Medical records of 385 ELBWIs with whole milk feeding, and freeze-thawed or pasteurized breast milk feeding were reviewed retrospectively. Postnatally acquired CMV infection was defined as an initial negative and a subsequent positive on follow-up urine CMV DNA polymerase chain reaction screening tests. The incidence, clinical characteristics, symptoms, sequelae, and long-term outcome at corrected age [(CA): 2 years of CMV infection] were analyzed.
RESULTS
While no infant developed CMV infection with whole milk (0/22) or pasteurized breast milk (0/62) feeding, postnatal CMV infection was diagnosed in 8% (27/301) of ELBWIs who were fed freeze-thawed breast milk. Gestational age in the CMV group was significantly lower than the control group. In 82% (22/27) of cases, CMV infection was symptomatic and was associated with increased ventilator days and > or =moderate bronchopulmonary dysplasia (BPD). Neurodevelopmental outcome and growth status at CA 2 years were not different between the study groups. Lower gestational age and freeze-thawed breast milk feeding >60% of total oral intake during the first 8 postnatal weeks were independent risk factors for acquiring postnatal CMV infection. BPD (> or =moderate) was the only significant adverse outcome associated with this CMV infection.
CONCLUSION
Pasteurization but not freeze-thawing of breast milk eradicated the postnatal acquisition of CMV infection through breast milk.
MeSH Terms
-
Adult
Breast Feeding
Bronchopulmonary Dysplasia
Cytomegalovirus/*isolation & purification
Cytomegalovirus Infections/epidemiology/prevention & control/*transmission
Female
Gestational Age
Humans
Incidence
Infant
*Infant, Extremely Low Birth Weight
Infant, Newborn
Infectious Disease Transmission, Vertical/*prevention & control
Male
Milk, Human/chemistry/*virology
Polymerase Chain Reaction
Pregnancy
Pregnancy Complications, Infectious/diagnosis
Retrospective Studies
Risk Factors
Figure
-
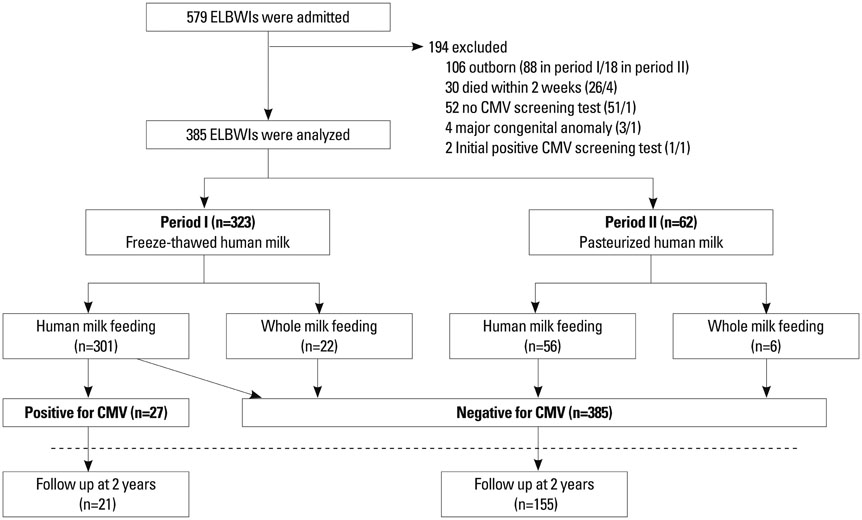
Fig. 1 Diagram showing enrollment and follow up of study patients during period I and II. ELBWI, extremely low birth weight infant; CMV, cytomegalovirus.
Cited by 1 articles
-
Incidence of Postnatal CMV Infection among Breastfed Preterm Infants: a Systematic Review and Meta-analysis
Hye Won Park, Myung Hyun Cho, Sun Hwan Bae, Ran Lee, Kyo Sun Kim
J Korean Med Sci. 2021;36(12):e84. doi: 10.3346/jkms.2021.36.e84.
Reference
-
1. Lawrence RA. The evidence for growth standards and iron in moderation and exclusive breastfeeding. Breastfeed Med. 2006; 1:205–206.
Article2. Hamprecht K, Maschmann J, Jahn G, Poets CF, Goelz R. Cytomegalovirus transmission to preterm infants during lactation. J Clin Virol. 2008; 41:198–205.
Article3. Vohr BR, Poindexter BB, Dusick AM, McKinley LT, Higgins RD, Langer JC, et al. Persistent beneficial effects of breast milk ingested in the neonatal intensive care unit on outcomes of extremely low birth weight infants at 30 months of age. Pediatrics. 2007; 120:e953–e959.
Article4. Dougherty D, Luther M. Birth to breast--a feeding care map for the NICU: helping the extremely low birth weight infant navigate the course. Neonatal Netw. 2008; 27:371–377.
Article5. Nijman J, de Vries LS, Koopman-Esseboom C, Uiterwaal CS, van Loon AM, Verboon-Maciolek MA. Postnatally acquired cytomegalovirus infection in preterm infants: a prospective study on risk factors and cranial ultrasound findings. Arch Dis Child Fetal Neonatal Ed. 2012; 97:F259–F263.
Article6. Numazaki K. Human cytomegalovirus infection of breast milk. FEMS Immunol Med Microbiol. 1997; 18:91–98.
Article7. Vochem M, Hamprecht K, Jahn G, Speer CP. Transmission of cytomegalovirus to preterm infants through breast milk. Pediatr Infect Dis J. 1998; 17:53–58.
Article8. Hamprecht K, Maschmann J, Vochem M, Dietz K, Speer CP, Jahn G. Epidemiology of transmission of cytomegalovirus from mother to preterm infant by breastfeeding. Lancet. 2001; 357:513–518.
Article9. Bae CW. Maternal diseases and breastfeeding. Hanyang Med Rev. 2010; 30:60–67.
Article10. Dworsky M, Stagno S, Pass RF, Cassady G, Alford C. Persistence of cytomegalovirus in human milk after storage. J Pediatr. 1982; 101:440–443.
Article11. Friis H, Andersen HK. Rate of inactivation of cytomegalovirus in raw banked milk during storage at -20 degrees C and pasteurisation. Br Med J (Clin Res Ed). 1982; 285:1604–1605.
Article12. Hamprecht K, Maschmann J, Müller D, Dietz K, Besenthal I, Goelz R, et al. Cytomegalovirus (CMV) inactivation in breast milk: reassessment of pasteurization and freeze-thawing. Pediatr Res. 2004; 56:529–535.
Article13. Ewaschuk JB, Unger S, O'Connor DL, Stone D, Harvey S, Clandinin MT, et al. Effect of pasteurization on selected immune components of donated human breast milk. J Perinatol. 2011; 31:593–598.
Article14. Maschmann J, Hamprecht K, Weissbrich B, Dietz K, Jahn G, Speer CP. Freeze-thawing of breast milk does not prevent cytomegalovirus transmission to a preterm infant. Arch Dis Child Fetal Neonatal Ed. 2006; 91:F288–F290.
Article15. Schanler RJ. Suitability of human milk for the low-birthweight infant. Clin Perinatol. 1995; 22:207–222.
Article16. Yoo HS, Shin JH, Jung UJ, Kim JK, Ahn SY, Kim ES, et al. Perinatal cytomegalovirus infection associated with freeze-thawed breast milk feeding in extremely low birth weight infants (<1000 gm). Denver: In SPR (Society for Pediatric Research);2009.17. Klein JO, Wilson CB, Nizet V, Maldonado YA. Infectious Diseases of the Fetus and Newborn Infant. 7th ed. Philadelphia: Elsevier;2011.18. Ehrenkranz RA, Walsh MC, Vohr BR, Jobe AH, Wright LL, Fanaroff AA, et al. Validation of the National Institutes of Health consensus definition of bronchopulmonary dysplasia. Pediatrics. 2005; 116:1353–1360.
Article19. Papile LA, Burstein J, Burstein R, Koffler H. Incidence and evolution of subependymal and intraventricular hemorrhage: a study of infants with birth weights less than 1,500 gm. J Pediatr. 1978; 92:529–534.
Article20. Bell MJ, Ternberg JL, Feigin RD, Keating JP, Marshall R, Barton L, et al. Neonatal necrotizing enterocolitis. Therapeutic decisions based upon clinical staging. Ann Surg. 1978; 187:1–7.21. The Committee for the Classification of Retinopathy of Prematurity. An international classification of retinopathy of prematurity. Arch Ophthalmol. 1984; 102:1130–1134.22. Leonard CH, Piecuch RE, Cooper BA. Use of the Bayley Infant Neurodevelopmental Screener with low birth weight infants. J Pediatr Psychol. 2001; 26:33–40.
Article23. Shankaran S, Johnson Y, Langer JC, Vohr BR, Fanaroff AA, Wright LL, et al. Outcome of extremely-low-birth-weight infants at highest risk: gestational age < or =24 weeks, birth weight < or =750 g, and 1-minute Apgar < or =3. Am J Obstet Gynecol. 2004; 191:1084–1091.
Article24. Ancel PY, Livinec F, Larroque B, Marret S, Arnaud C, Pierrat V, et al. Cerebral palsy among very preterm children in relation to gestational age and neonatal ultrasound abnormalities: the EPIPAGE cohort study. Pediatrics. 2006; 117:828–835.
Article25. Maschmann J, Hamprecht K, Dietz K, Jahn G, Speer CP. Cytomegalovirus infection of extremely low-birth weight infants via breast milk. Clin Infect Dis. 2001; 33:1998–2003.
Article26. Nijman J, van Loon AM, de Vries LS, Koopman-Esseboom C, Groenendaal F, Uiterwaal CS, et al. Urine viral load and correlation with disease severity in infants with congenital or postnatal cytomegalovirus infection. J Clin Virol. 2012; 54:121–124.
Article27. Hayashi S, Kimura H, Oshiro M, Kato Y, Yasuda A, Suzuki C, et al. Transmission of cytomegalovirus via breast milk in extremely premature infants. J Perinatol. 2011; 31:440–445.
Article28. Okulu E, Akin IM, Atasay B, Ciftçi E, Arsan S, Türmen T. Severe postnatal cytomegalovirus infection with multisystem involvement in an extremely low birth weight infant. J Perinatol. 2012; 32:72–74.
Article29. Hamprecht K, Witzel S, Maschmann J, Dietz K, Baumeister A, Mikeler E, et al. Rapid detection and quantification of cell free cytomegalovirus by a high-speed centrifugation-based microculture assay: comparison to longitudinally analyzed viral DNA load and pp67 late transcript during lactation. J Clin Virol. 2003; 28:303–316.
Article30. Jim WT, Shu CH, Chiu NC, Chang JH, Hung HY, Peng CC, et al. High cytomegalovirus load and prolonged virus excretion in breast milk increase risk for viral acquisition by very low birth weight infants. Pediatr Infect Dis J. 2009; 28:891–894.
Article31. Mussi-Pinhata MM, Pinto PC, Yamamoto AY, Berencsi K, de Souza CB, Andrea M, et al. Placental transfer of naturally acquired, maternal cytomegalovirus antibodies in term and preterm neonates. J Med Virol. 2003; 69:232–239.
Article32. Palmeira P, Quinello C, Silveira-Lessa AL, Zago CA, Carneiro-Sampaio M. IgG placental transfer in healthy and pathological pregnancies. Clin Dev Immunol. 2012; 2012:985646.
Article33. Doctor S, Friedman S, Dunn MS, Asztalos EV, Wylie L, Mazzulli T, et al. Cytomegalovirus transmission to extremely low-birthweight infants through breast milk. Acta Paediatr. 2005; 94:53–58.
Article34. Capretti MG, Lanari M, Lazzarotto T, Gabrielli L, Pignatelli S, Corvaglia L, et al. Very low birth weight infants born to cytomegalovirus-seropositive mothers fed with their mother's milk: a prospective study. J Pediatr. 2009; 154:842–848.
Article35. Cheong JL, Cowan FM, Modi N. Gastrointestinal manifestations of postnatal cytomegalovirus infection in infants admitted to a neonatal intensive care unit over a five year period. Arch Dis Child Fetal Neonatal Ed. 2004; 89:F367–F369.
Article36. Arellano-Galindo J, Villanueva-García D, Cruz-Ramirez JL, Yalaupari-Mejìa JP, Uribe-Gutiérrez G, Velazquez-Guadarrama N, et al. Detection and gB genotyping of CMV in Mexican preterm infants in the context of maternal seropositivity. J Infect Dev Ctries. 2014; 8:758–767.
Article37. Mehler K, Oberthuer A, Lang-Roth R, Kribs A. High rate of symptomatic cytomegalovirus infection in extremely low gestational age preterm infants of 22-24 weeks' gestation after transmission via breast milk. Neonatology. 2014; 105:27–32.
Article38. Yeager AS, Grumet FC, Hafleigh EB, Arvin AM, Bradley JS, Prober CG. Prevention of transfusion-acquired cytomegalovirus infections in newborn infants. J Pediatr. 1981; 98:281–287.
Article39. Snydman DR, Werner BG, Meissner HC, Cheeseman SH, Schwab J, Bednarek F, et al. Use of cytomegalovirus immunoglobulin in multiply transfused premature neonates. Pediatr Infect Dis J. 1995; 14:34–40.
Article40. Kurath S, Halwachs-Baumann G, Müller W, Resch B. Transmission of cytomegalovirus via breast milk to the prematurely born infant: a systematic review. Clin Microbiol Infect. 2010; 16:1172–1178.
Article41. Jim WT, Shu CH, Chiu NC, Kao HA, Hung HY, Chang JH, et al. Transmission of cytomegalovirus from mothers to preterm infants by breast milk. Pediatr Infect Dis J. 2004; 23:848–851.
Article42. Mussi-Pinhata MM, Yamamoto AY, do Carmo Rego MA, Pinto PC, da Motta MS, Calixto C. Perinatal or early-postnatal cytomegalovirus infection in preterm infants under 34 weeks gestation born to CMV-seropositive mothers within a high-seroprevalence population. J Pediatr. 2004; 145:685–688.
Article43. Yasuda A, Kimura H, Hayakawa M, Ohshiro M, Kato Y, Matsuura O, et al. Evaluation of cytomegalovirus infections transmitted via breast milk in preterm infants with a real-time polymerase chain reaction assay. Pediatrics. 2003; 111(6 Pt 1):1333–1336.
Article44. Meier J, Lienicke U, Tschirch E, Krüger DH, Wauer RR, Prösch S. Human cytomegalovirus reactivation during lactation and mother-to-child transmission in preterm infants. J Clin Microbiol. 2005; 43:1318–1324.
Article45. Ford JE, Law BA, Marshall VM, Reiter B. Influence of the heat treatment of human milk on some of its protective constituents. J Pediatr. 1977; 90:29–35.
Article46. Goldblum RM, Dill CW, Albrecht TB, Alford ES, Garza C, Goldman AS. Rapid high-temperature treatment of human milk. J Pediatr. 1984; 104:380–385.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Postnatal cytomegalovirus infection in an extremely premature infant transmitted via breast milk: A case report
- Incidence of Postnatal CMV Infection among Breastfed Preterm Infants: a Systematic Review and Meta-analysis
- Effective Strategies for the Prevention of Nosocomial Sepsis in Extremely Premature Infants
- Clinical Findings According to Feeding Diets in Very Low Birth Weight Infants: Human Breast Milk versus Bovine Milk-Based Formula
- Central Diabetes Insipidus Associated with Symptomatic Cytomegalovirus Infection in an Extremely Low Birth Weight Infant
