J Dent Anesth Pain Med.
2016 Dec;16(4):309-312. 10.17245/jdapm.2016.16.4.309.
Pharyngeal flap damage caused by nasotracheal intubation in a patient who underwent palatoplasty and pharyngoplasty
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Pusan National University, Yangsan, Korea.
- 2Department of Dental Anesthesia and Pain Medicine, Pusan National University Dental Hospital, Dental Research Institute, Yangsan, Korea. dryoonji@pusan.ac.kr
- 3Department of Anesthesia and Pain Medicine, Pusan National University Yangsan Hospital, Yangsan, Korea.
- KMID: 2366160
- DOI: http://doi.org/10.17245/jdapm.2016.16.4.309
Abstract
- Patients with cleft lip and palate (CLP) must undergo corrective surgeries during infancy and early childhood. Many patients with CLP undergo orthognathic surgery during their childhood for correction of skeletal asymmetries or pharyngoplasty with a pharyngeal flap to improve the quality of speech and velopharyngeal function. During orthognathic surgeries, nasotracheal intubation is performed under general anesthesia. In our case report, the patient had undergone palatoplasty and pharygoplasty previously. During the orthognathic surgery, a flexible fiberoptic bronchoscope-guided nasotracheal tube was inserted through the pharyngeal flap ostium; however, active bleeding occurred in the nasopharynx. Bleeding occurred because the flap was torn. After achieving hemostasis, the surgery was completed successfully. Thus, if a patient may show the potential for velopharyngeal port obstruction, nasotracheal intubation should be performed with utmost care.
Keyword
MeSH Terms
Figure
-
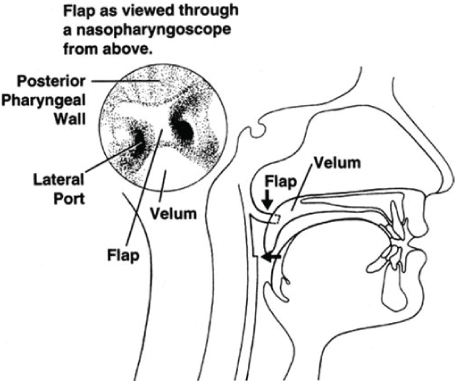
Fig. 1 Nasopharyngoscopic view of velopharyngeal port and flap.

Fig. 2 Postoperative nasendoscopic examnination shows intact pharyngeal flap (arrow).
Reference
-
1. Kopp VJ, Rosenfeld MJ, Turvey TA. Nasotracheal intubation in the presence of pharyngeal flap in children and adults. Anesthesiology. 1995; 82:1063–1064.
Article2. Hee HI, Conskunfirat ND, Wong SY, Chen C. Airway management in a patient with a cleft palate after pharyngoplasty: a case report. Can J Anesth. 2003; 50:721–724.
Article3. Panula K, Lovius BB, Pospisil OA. The need for orthognathic surgery in patients born with complete cleft palate or complete unilateral cleft lip and palate. Oral Surg Oral Diagn. 1993; 4:23–28.
Article4. Davies D. Cleft lip and palate. British Medical Journal. 1985; 290:625–628.
Article5. Bell CN, Macintyre DR, Ross JW, Pigott RW, Weller RM. Pharyngoplasty: a hazard for nasotracheal intubation. Br J Oral Maxillofac Surg. 1986; 24:212–216.
Article6. Robin NH, Baty H, Franklin J, Guyton FC, Mann J, Woolley AL, et al. The multidisciplinary evaluation and management of cleft lip and palate. South Med J. 2006; 99:1111–1120.
Article7. Piepho T, Thierbach A, Werner C. Nasotracheal intubation: look before you leap. Br J Anaesth. 2005; 94:859–860.
Article8. Enk D, Palmes AM, Van Aken H, Westphal M. Nasotracheal intubation: a simple and effective technique to reduce nasopharyngeal trauma and tube contamination. Anesth Analg. 2002; 95:1432–1436.
Article9. Kihara S, Komatsuzaki T, Brimacombe JR, Yaguchi Y, Taguchi N, Watanabe S. A silicone-based wire-reinforced tracheal tube with a hemispherical bevel reduces nasal morbidity for nasotracheal intubation. Anesth Analg. 2003; 97:1488–1491.10. Hansen M, Poulsen MR, Bendixen DK, Hartmann-Andersen F. Incidence of sinusitis in patients with nasotracheal intubation. Br J Anaesth. 1988; 61:231–232.11. Onçag O, Cokmez B, Aydemir S, Balcioglu T. Investigation of bacteremia following nasotracheal intubation. Paediatr Anaesth. 2005; 15:194–198.
Article12. Ng SY, Yew WS. Nasotracheal tube occlusion from adenoid trauma. Anaesth Intensive Care. 2006; 34:829–830.
Article13. Krebs MJ, Sakai T. Retropharyngeal dissection during nasotracheal intubation: a rare complication and its Management. J Clin Anesth. 2008; 20:218–221.
Article14. Kim YC, Lee SH, Noh GJ, Cho SY, Yeom JH, Shin WJ. Thermosoftening Treatment of the nasotracheal tube before intubation can reduce epistaxis and nasal damage. Anesth Analg. 2000; 91:698–701.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- The Analysis on Degree of Discomfort Caused by Delayed Extubation of Nasotracheal Tube: A Pilot Study
- Retropharyngeal Dissection during Nasotracheal Intubation: A Case Report
- Effective removal of epistaxis during nasotracheal intubation utilizing a fiberoptic scope in a difficult airway: A case report
- Use of the Airtraq(R) optical laryngoscope as a rescue airway device following failed awake flexible fiberoptic nasotracheal intubation of a patient with severe microsomia: A case report
- The Effect of Laryngeal View Grade and Intraoral Bleeding on Intubation Difficulty during Fiberoptic Nasotracheal Intubation
