Evaluation of Fragment Reduction Feasibility When Treating Bony Mallet Finger Using Extension Block K-Wire Technique
- Affiliations
-
- 1Armed Forces Yangju Hospital, Yangju, Korea.
- 2Department of Orthopaedic Surgery, Seoul National University Hospital, Seoul, Korea. seroobin@naver.com
- KMID: 2364212
- DOI: http://doi.org/10.12790/jkssh.2016.21.4.212
Abstract
- PURPOSE
The purpose was to evaluate fragment reduction feasilibty when applying extension block Kirschner-wire technique for bony mallet finger.
METHODS
We treated 48 displaced mallet finger fractures by a two extension block Kirschner-wire technique. Among these operation group, we found dorsal rotation of fragment in 18 cases, making it difficult to get anatomical reduction. The patients were divided into two groups. One group of 30 patients did not show dorsal rotation of fragment and anatomical reduction was achieved easily. Another group of 18 patients showed dorsal rotation of fragment and additional methods was applied to achieve anatomical reduction.
RESULTS
Joint surface involvement was significant greater in groups showing dorsal rotation of fragment than group which did not show (57.1% and 49.7%, respectively) (p=0.01). The groups whose joint surface involvement more than 50% had higher risk of dorsal rotation of fragment than the group less than 50%, with the odds ratio of 6.11.
CONCLUSION
We could encounter the cases which showed dorsal rotation of the fracture fragment when treating the bony mallet finger with extension block K-wire technique especially the joint surface involvement was more than 50%. So if we can evaluate the extents of joint surface involvement and prepare additional method preoperatively when dorsal rotation of fragment is expected, it is possible to get more favorable results.
MeSH Terms
Figure
-
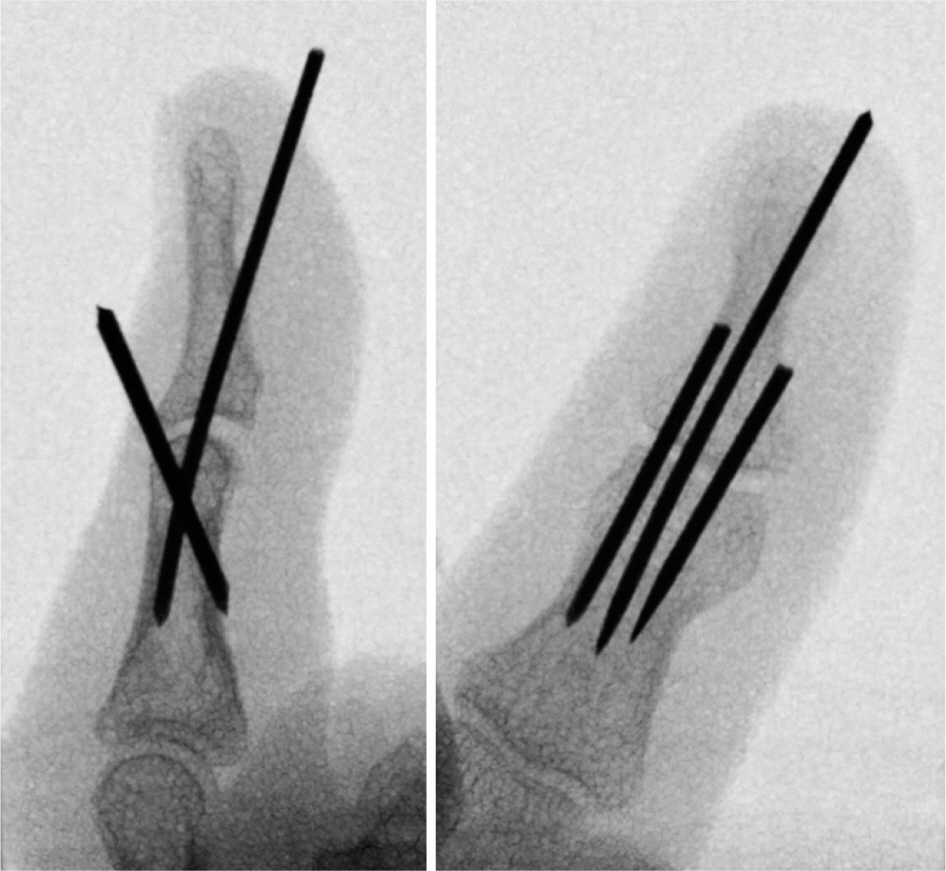
Fig. 1. A 24-year-old woman has a bony mallet finger injury of little finger. Intraoperative C-arm image with two extension block K-wire technique10.

Fig. 2. (A) Bony mallet finger injury showing 42% of joint surface involvement. (B) Anatomical reduction was achieved without dorsal rotation of fragment by two-extension block technique.

Fig. 3. (A) Bony mallet finger injury showing 51.7% of joint surface involvement. (B) Dorsal rotation of fragment was noted even though two-extension block technique.
Cited by 1 articles
-
Alternative Technique Using Opencast for Early Return to Play after Operation in Patients with Bony Mallet Finger by Sports Injury: A Retrospective Study in a Tertiary Hospital in South Korea
Kyung Ho Lee, Sung Yoon Jung, Ji Woong Kim
Korean J Sports Med. 2024;42(2):113-118. doi: 10.5763/kjsm.2024.42.2.113.
Reference
-
1. Stark HH, Gainor BJ, Ashworth CR, Zemel NP, Rickard TA. Operative treatment of intra-articular fractures of the dorsal aspect of the distal phalanx of digits. J Bone Joint Surg Am. 1987; 69:892–6.
Article2. Bischoff R, Buechler U, De Roche R, Jupiter J. Clinical results of tension band fixation of avulsion fractures of the hand. J Hand Surg Am. 1994; 19:1019–26.
Article3. Damron TA, Engber WD. Surgical treatment of mallet finger fractures by tension band technique. Clin Orthop Relat Res. 1994; (300):133–40.
Article4. Hamas RS, Horrell ED, Pierret GP. Treatment of mallet finger due to intra-articular fracture of the distal phalanx. J Hand Surg Am. 1978; 3:361–3.
Article5. Ishiguro T, Inoue K, Matsubayashi N, Ito Y, Hashizume N. A new method of closed reduction for mallet fractures. J Jpn Soc Surg Hand. 1988; 5:444–7.6. Hofmeister EP, Mazurek MT, Shin AY, Bishop AT. Extension block pinning for large mallet fractures. J Hand Surg Am. 2003; 28:453–9.
Article7. Shimura H, Wakabayashi Y, Nimura A. A novel closed reduction with extension block and flexion block using Kirschner wires and microscrew fixation for mallet fractures. J Orthop Sci. 2014; 19:308–12.
Article8. Zhang W, Zhang X, Zhao G, Gao S, Yu Z. Pressing fixation of mallet finger fractures with the end of a K-wire (a new fixation technique for mallet fractures). Injury. 2016; 47:377–82.
Article9. King HJ, Shin SJ, Kang ES. Complications of operative treatment for mallet fractures of the distal phalanx. J Hand Surg Br. 2001; 26:28–31.10. Lee YH, Kim JY, Chung MS, Baek GH, Gong HS, Lee SK. Two extension block Kirschner wire technique for mallet finger fractures. J Bone Joint Surg Br. 2009; 91:1478–81.
Article11. Wehbe MA, Schneider LH. Mallet fractures. J Bone Joint Surg Am. 1984; 66:658–69.12. Konishiike T, Kodota Y, Hashizume H. Fracture pattern of bony mallet fingers. J Jpn Soc Surg Hand. 2006; 23:496–500.13. Kim JY, Lee SH. Factors Related to Distal Interphalangeal Joint Extension Loss After Extension Block Pinning of Mallet Finger Fractures. J Hand Surg Am. 2016; 41:414–9.
Article14. Han KJ, Moon JH, Chung NS, Kang SY. Treatment of mallet fracture of the fingers by percutaneous reduction and pinning. J Korean Soc Surg Hand. 2003; 8:153–7.15. Shin HD, Kim KC, Yang JH, Kim BK. Mallet fracture of percutaneous small-screw fixation after closed reduction. J Korean Soc Surg Hand. 2008; 13:288–93.16. Park HC, Park HS, Ahn SC, Kim SS, Chang J. Modified extension block technique using conjoined Kirschner wires for bony mallet fingers. J Korean Soc Surg Hand. 2010; 15:164–8.17. Jeon HS, Jeon SJ, Moon CS, Jung SH, Jeon SK. Closed reduction and percutaneous K-wire fixation of bony mallet finger using an 18 gauge needle. J Korean Soc Surg Hand. 2010; 15:77–82.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Prognostic Factors of the Extension Block Technique for the Bony Mallet Finger
- Treatment of Bony Mallet Finger: Closed Reduction Using Extension Block K-wire
- Closed Reduction of Mallet Fractures using Extension Black Kirshner Wire
- The Result of the Modified Extension Block Technique in Bony Mallet Finger
- Reduction Loss after Extension Block Kirschner Wire Fixation for Treatment of Bony Mallet Finger
