Computer-Assisted Rotational Acetabular Osteotomy for Patients with Acetabular Dysplasia
- Affiliations
-
- 1Department of Orthopaedic Surgery, Yokohama City University, Yokohama, Japan. yute0131@med.yokohama-cu.ac.jp
- KMID: 2363952
- DOI: http://doi.org/10.4055/cios.2016.8.1.99
Abstract
- Rotational acetabular osteotomy (RAO) is a well-established surgical procedure for patients with acetabular dysplasia, and excellent long-term results have been reported. However, RAO is technically demanding and precise execution of this procedure requires experience with this surgery. The usefulness of computer navigation in RAO includes its ability to perform three-dimensional (3D) preoperative planning, enable safe osteotomy even with a poor visual field, reduce exposure to radiation from intraoperative fluoroscopy, and display the tip position of the chisel in real time, which is educationally useful as it allows staff other than the operator to follow the progress of the surgery. In our results comparing 23 hips that underwent RAO with navigation and 23 hips operated on without navigation, no significant difference in radiological assessment was observed. However, no perioperative complications were observed in the navigation group whereas one case of transient femoral nerve palsy was observed in non-navigation group. A more accurate and safer RAO can be performed using 3D preoperative planning and intraoperative assistance with a computed tomography-based navigation system.
MeSH Terms
Figure
-
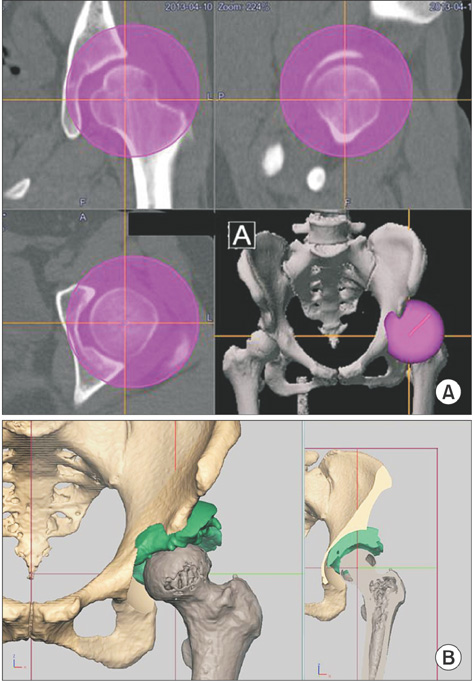
Fig. 1 Preoperative planning of rotational acetabular osteotomy using computer software. (A) In the preoperative planning of the osteotomy line, spherical osteotomy of the acetabulum is planned so that the center of the sphere is near the center of the femoral head (or the center of the hip joint). (B) The plan is to rotate it laterally until the acetabular roof obliquity angle becomes 0° and the anterior coverage is corrected.
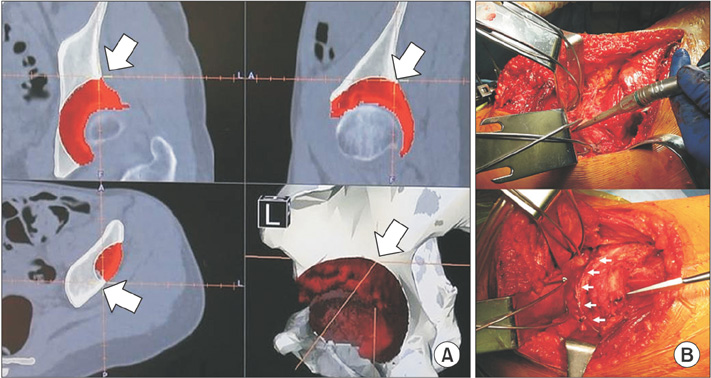
Fig. 2 Marking of the osteotomy line using a registered high-speed drill. (A) The tip position of the high-speed drill can be confirmed on the computer screen during surgery (arrow: the intersection of two orange lines). (B) The osteotomy line is marked with the high-speed drill according to the preoperative plan while the position of the tip of the high-speed drill is confirmed (arrows).
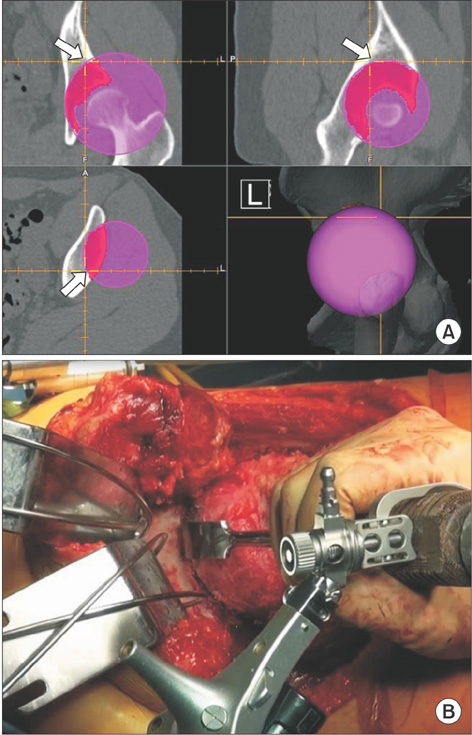
Fig. 3 Osteotomy using a registered curved chisel. (A) The tip position of the curved chisel can be confirmed on the computer screen during surgery (arrow: the intersection of two orange lines). (B) Osteotomy is performed according to the preoperative plan with real-time image guidance.
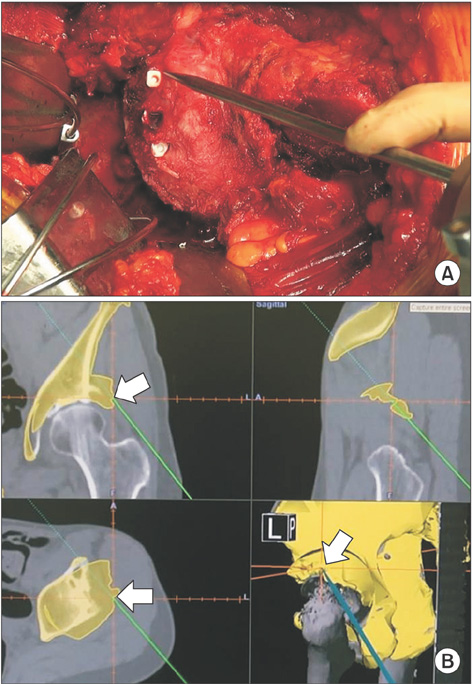
Fig. 4 Confirmation of position after transposition of the bone fragment. (A) By touching the surface of the rotated bone fragment with a pointer after rotating the bone fragment obtained by osteotomy and fixing it with three polylactic acid absorbable screws, it is confirmed whether or not the position fits the surface of the planned position after rotation in the preoperative plan. (B) The arrow shows the pointer tip, which touches the surface of the rotated bone fragment at the same position as in the preoperative plan (yellow portion).
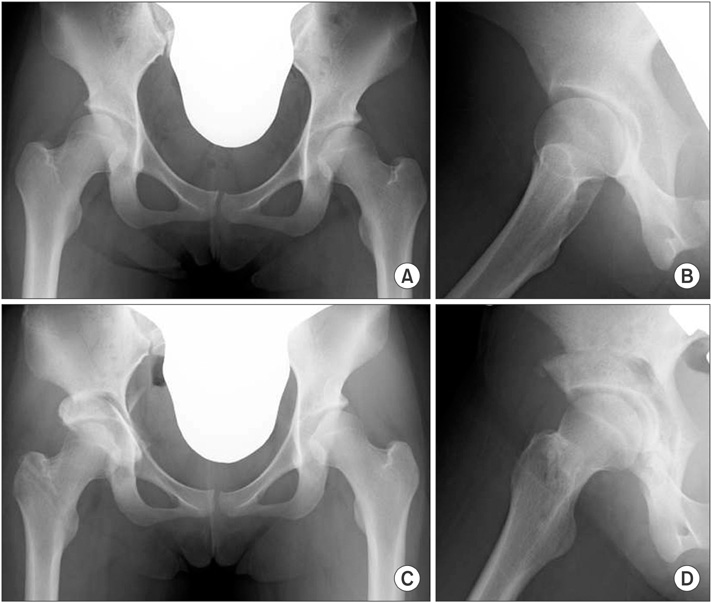
Fig. 5 Case presentation of rotational acetabular osteotomy using a computed tomography (CT)-based navigation. A female patient aged 19 years with bilateral acetabular dysplasia. Rotational acetabular osteotomy of the right hip was performed using a CT-based navigation system. The acetabular head index (AHI) was 68%, center-edge (CE) angle was 10°, and acetabular roof angle was 21° in the right hip preoperatively; these improved to AHI of 92%, CE angle of 40°, and acetabular roof angle of 0° postoperatively. (A) Preoperative frontal radiograph of both hips. (B) Preoperative lateral radiograph of the right hip. (C) Frontal radiograph of both hips at 6 weeks postoperatively. (D) Lateral radiograph of the right hip at 6 weeks postoperatively.
Reference
-
1. Ninomiya S, Tagawa H. Rotational acetabular osteotomy for the dysplastic hip. J Bone Joint Surg Am. 1984; 66(3):430–436.
Article2. Nozawa M, Shitoto K, Matsuda K, Maezawa K, Kurosawa H. Rotational acetabular osteotomy for acetabular dysplasia: a follow-up for more than ten years. J Bone Joint Surg Br. 2002; 84(1):59–65.3. Takatori Y, Ninomiya S, Nakamura S, et al. Long-term results of rotational acetabular osteotomy in patients with slight narrowing of the joint space on preoperative radiographic findings. J Orthop Sci. 2001; 6(2):137–140.
Article4. Massie WK, Howorth MB. Congenital dislocation of the hip. Part I: method of grading results. J Bone Joint Surg Am. 1950; 32(3):519–531.5. Iwana D, Nakamura N, Miki H, Kitada M, Hananouchi T, Sugano N. Accuracy of angle and position of the cup using computed tomography-based navigation systems in total hip arthroplasty. Comput Aided Surg. 2013; 18(5-6):187–194.
Article6. Akiyama H, Goto K, So K, Nakamura T. Computed tomography-based navigation for curved periacetabular osteotomy. J Orthop Sci. 2010; 15(6):829–833.
Article7. Langlotz F, Bachler R, Berlemann U, Nolte LP, Ganz R. Computer assistance for pelvic osteotomies. Clin Orthop Relat Res. 1998; (354):92–102.
Article8. Hsieh PH, Chang YH, Shih CH. Image-guided periacetabular osteotomy: computer-assisted navigation compared with the conventional technique: a randomized study of 36 patients followed for 2 years. Acta Orthop. 2006; 77(4):591–597.
Article9. Tokunaga K, Watanabe K. Accuracy of the surface-match registration on the inner table of the pelvis in the CT-based navigation for the curved periacetabular osteotomy. Hip Joint. 2012; 38:161–165.10. Tsumura H, Kaku N, Ikeda S, Torisu T. A computer simulation of rotational acetabular osteotomy for dysplastic hip joint: does the optimal transposition of the acetabular fragment exist. J Orthop Sci. 2005; 10(2):145–151.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Stress Distribution According to Center-Edge Angle in Dysplastic Hip and the Biomechanical Effect of Rotational Acetabular Osteotomy
- Rotational acetabular osteotomy in acetabular dysplasia
- Rotational Acetabular Osteotomy for the Dysplastic Hip: A Follow-up for 5 to 18 years
- Rotational Acetabular Osteotomy for the Dysplastic Acetabulum
- Rotational Acetabular Osteotomy
