Clin Exp Otorhinolaryngol.
2015 Jun;8(2):161-166. 10.3342/ceo.2015.8.2.161.
Changes in the Flow-Volume Curve According to the Degree of Stenosis in Patients With Unilateral Main Bronchial Stenosis
- Affiliations
-
- 1Department of Pulmonary and Critical Care Medicine, Hallym University Kangdong Sacred Heart Hospital, Seoul, Korea. hjk3425@skku.edu
- 2Korea Institute for Industrial Economics and Trade, Seoul, Korea.
- 3Department of Radiology, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea.
- 4Division of Pulmonary and Critical Care Medicine, Department of Medicine, Samsung Medical Center, Sungkyunkwan University School of Medicine, Seoul, Korea. hjk3425@skku.edu
- KMID: 2360788
- DOI: http://doi.org/10.3342/ceo.2015.8.2.161
Abstract
OBJECTIVES
The shape of the flow-volume (F-V) curve is known to change to showing a prominent plateau as stenosis progresses in patients with tracheal stenosis. However, no study has evaluated changes in the F-V curve according to the degree of bronchial stenosis in patients with unilateral main bronchial stenosis.
METHODS
We performed an analysis of F-V curves in 29 patients with unilateral bronchial stenosis with the aid of a graphic digitizer between January 2005 and December 2011.
RESULTS
The primary diseases causing unilateral main bronchial stenosis were endobronchial tuberculosis (86%), followed by benign bronchial tumor (10%), and carcinoid (3%). All unilateral main bronchial stenoses were classified into one of five grades (I, < or =25%; II, 26%-50%; III, 51%-75%; IV, 76%-90%; V, >90% to near-complete obstruction without ipsilateral lung collapse). A monophasic F-V curve was observed in patients with grade I stenosis and biphasic curves were observed for grade II-IV stenosis. Both monophasic (81%) and biphasic shapes (18%) were observed in grade V stenosis. After standardization of the biphasic shape of the F-V curve, the breakpoints of the biphasic curve moved in the direction of high volume (x-axis) and low flow (y-axis) according to the progression of stenosis.
CONCLUSION
In unilateral bronchial stenosis, a biphasic F-V curve appeared when bronchial stenosis was >25% and disappeared when obstruction was near complete. In addition, the breakpoint moved in the direction of high volume and low flow with the progression of stenosis.
MeSH Terms
Figure
-
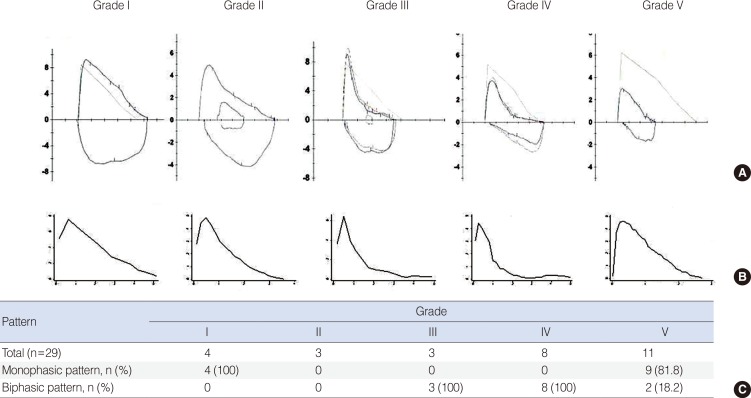
Fig. 1 Representative cases (A), median graph (B), and the expiratory pattern of the flow-volume curve (C) according to the degree of stenosis.

Fig. 2 Standardized graph using the median value of the breakpoint according to the degree of stenosis. The more advanced the unilateral bronchial stenosis, the more the breakpoint moved from top to bottom and from inside to outside on the x-axis (volume) and y-axis (flow), respectively. F-V, flow-volume; FVC, forced vital capacity.
Reference
-
1. Murray JF, Mason RJ. Murray and Nadel's textbook of respiratory medicine. 5th ed. Philadelphia: Saunders Elsevier;2010.2. Pellegrino R, Viegi G, Brusasco V, Crapo RO, Burgos F, Casaburi R, et al. Interpretative strategies for lung function tests. Eur Respir J. 2005; 11. 26(5):948–968. PMID: 16264058.3. Husain A, Habib SS. Pattern identification of obstructive and restrictive ventilatory impairment through flow volume curves. Pak J Physiol. 2008; 5. 4(1):30–34.4. Miller RD, Hyatt RE. Obstructing lesions of the larynx and trachea: clinical and physiologic characteristics. Mayo Clin Proc. 1969; 3. 44(3):145–161. PMID: 5776050.5. Miller RD, Hyatt RE. Evaluation of obstructing lesions of the trachea and larynx by flow-volume loops. Am Rev Respir Dis. 1973; 9. 108(3):475–481. PMID: 4745245.6. Guntupalli KK, Bandi V, Sirgi C, Pope C, Rios A, Eschenbacher W. Usefulness of flow volume loops in emergency center and ICU settings. Chest. 1997; 2. 111(2):481–488. PMID: 9042000.
Article7. Gascoigne AD, Corris PA, Dark JH, Gibson GJ. The biphasic spirogram: a clue to unilateral narrowing of a mainstem bronchus. Thorax. 1990; 8. 45(8):637–638. PMID: 2099756.
Article8. Mazzei JA, Barro A, Mazzei ME, Portas T, Esteva H. Biphasic flow volume curve due to obstruction of main bronchus by bronchogenic cyst. Respir Med CME. 2011; 4(3):116–118.
Article9. Choi SJ, Jo MS, Lee HP, Kim JI, Yum HK. A case of biphasic flow-volume loop in left mainstem bronchial stenosis. Tuberc Respir Dis. 1998; 4. 45(2):416–420.
Article10. Roos CM, Braat MC. End-inspiratory flow reduction in the forced flow-volume curve as a sign of unilateral bronchial disease. Neth J Med. 1985; 28(10):378–382. PMID: 4080042.11. Breen PH, Serina ER, Barker SJ. Exhaled flow monitoring can detect bronchial flap-valve obstruction in a mechanical lung model. Anesth Analg. 1995; 8. 81(2):292–296. PMID: 7618717.
Article12. Anzueto A, Levine SM, Tillis WP, Calhoon JH, Bryan CL. Use of the flow-volume loop in the diagnosis of bronchial stenosis after single lung transplantation. Chest. 1994; 3. 105(3):934–936. PMID: 7510602.
Article13. Villaran Y, Sekela ME, Burki NK. Maximal expiratory flow patterns after single-lung transplantation in patients with and without chronic airways obstruction. Chest. 2001; 1. 119(1):163–168. PMID: 11157599.
Article14. Falzon D, Jaramillo E, Schünemann HJ, Arentz M, Bauer M, Bayona J, et al. WHO guidelines for the programmatic management of drug-resistant tuberculosis: 2011 update. Eur Respir J. 2011; 9. 38(3):516–528. PMID: 21828024.
Article15. Beauchemin C, Dixit NM, Perelson AS. Characterizing T cell movement within lymph nodes in the absence of antigen. J Immunol. 2007; 5. 178(9):5505–5512. PMID: 17442932.
Article16. Freitag L, Ernst A, Unger M, Kovitz K, Marquette CH. A proposed classification system of central airway stenosis. Eur Respir J. 2007; 7. 30(1):7–12. PMID: 17392320.
Article17. Gelb AF, Tashkin DP, Epstein JD, Szeftel A, Fairshter R. Physiologic characteristics of malignant unilateral main-stem bronchial obstruction: diagnosis and Nd-YAG laser treatment. Am Rev Respir Dis. 1988; 12. 138(6):1382–1385. PMID: 2462389.
Article18. Revelly JP, Feihl F, Liebling T, Perret C. Time constant histograms from the forced expired volume signal: a clinical evaluation. Eur Respir J. 1989; 6. 2(6):536–542. PMID: 2744137.19. Pimmel RL, Miller TK 3rd, Fouke JM, Eyles JG. Time-constant histograms from the forced expired volume signal. J Appl Physiol Respir Environ Exerc Physiol. 1981; 12. 51(6):1581–1593. PMID: 7319887.
Article20. Karkhanis VS, Joshi JM. Spirometry in chronic obstructive lung disease (COPD). J Assoc Physicians India. 2012; 2. 60(Suppl):22–26. PMID: 23155809.21. Low SY, Hsu A, Eng P. Interventional bronchoscopy for tuberculous tracheobronchial stenosis. Eur Respir J. 2004; 9. 24(3):345–347. PMID: 15358688.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Biphasic Flow-volume Loop in Left Mainstem Bronchial Stenosis
- Biphasic pattern of flow-volume curve (Unilateral main bronchus stenosis)
- Balloon dilatation of bronchial stenosis in adult
- A Case of Bronchial Varices in a Patient with Severe Mitral Stenosis
- A Case of Bronchial Stenosis due to Endotrcheal Suction
