The Neck and Posterior Fossa Combined Penetrating Injury: A Case Report
- Affiliations
-
- 1Department of Neurosurgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. ybkim69@yuhs.ac
- KMID: 2356797
- DOI: http://doi.org/10.13004/kjnt.2016.12.2.175
Abstract
- Here we report a case of penetrating neck injury to the posterior fossa that was shown, using high-resolution computed tomography (HRCT) and digital subtraction angiography (DSA), to involve no vascular injury. A 54-year-old man was brought to the emergency department after a penetrating injury to the left side of the posterior neck and occipital area with a knife. He was in an intoxicated state and could not communicate readily. On initial examination, his vital signs were stable and there was no active bleeding from the penetrating site. Because of concern about possible injury to adjacent vessels, we performed HRCT and DSA sequentially, and identified that the blade of the knife had just missed the arteriovenous structures in the neck and posterior fossa. The patient was then transferred to the operating room where the knife was gently removed. Further careful exploration was performed through the penetrating wound, and we confirmed that there were no major injuries to the vessels and neural structures. Postoperative computed tomography revealed that there was minimal hemorrhage in the left cerebellar hemisphere. The patient made a full recovery without any neurologic deficit. In this case, HRCT is a suitable tool for the initial overall evaluation. For the evaluation of vascular injury, DSA can be a specific and accurate tool. Mandatory exploration widely used for penetrating injuries. After careful preoperative evaluation and interpretation, simple withdrawal of material can be a choice of treatment.
MeSH Terms
Figure
-
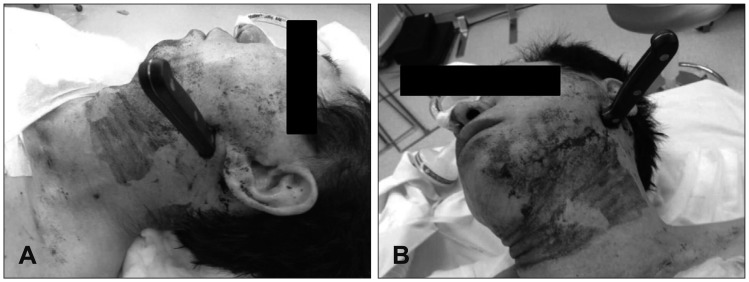
FIGURE 1 Photograph taken in the emergency room. (A) The knife is shown to be penetrating from behind the left mandible (B) toward the occiput.
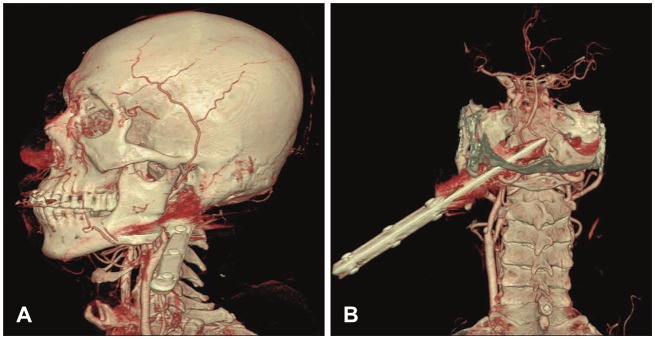
FIGURE 2 (A) Three-dimensional reconstructed computed tomography showing that the knife pierced the paraspinal muscles on the left side and (B) the base of the occipital bone behind the stylomastoid foramen.
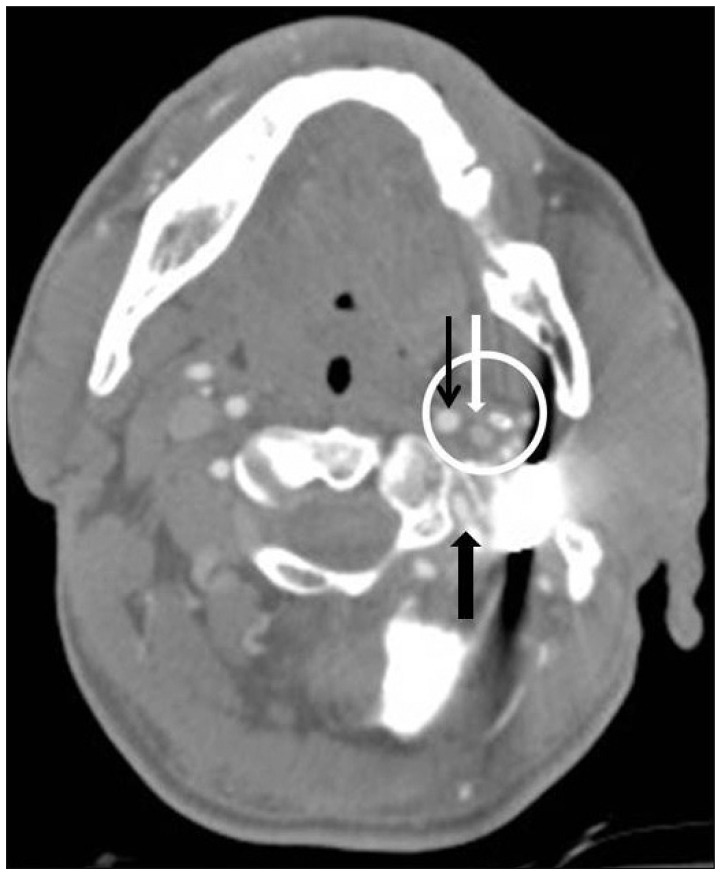
FIGURE 3 High-resolution computed tomography showing the major vessels (white circle) were a little apart from the blade of the penetrating knife. Internal carotid artery (narrow black arrow), internal jugular vein (white arrow), and vertebral artery (black arrow).
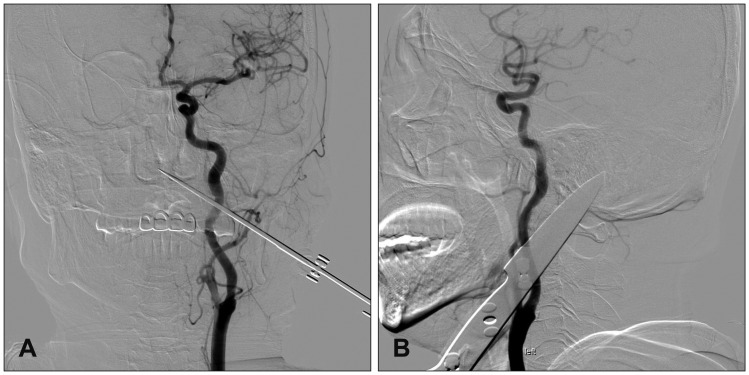
FIGURE 4 Injection of the left carotid artery in digital subtraction angiography showed a patent carotid artery; however, it is not clear if foreign material is pressing on the artery. (A) Anterior posterior projection (B), lateral projection.
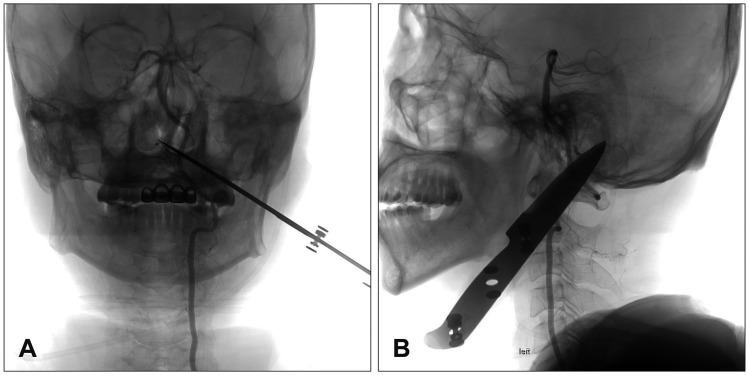
FIGURE 5 On digital subtraction angiography, injection of the left vertebral artery showed this vessel to be patent. (A) Anterior-posterior projection and (B) lateral projection.
Reference
-
1. Arabi B, Alden TD, Chesnut RM, Downs JH 3rd, Ecklund JM, Eisenberg HM, et al. Neuroimaging in the management of penetrating brain injury. J Trauma. 2001; 51:S7–S11. PMID: 11505193.2. Bell RB, Dierks EJ, Homer L, Potter BE. Management of cerebrospinal fluid leak associated with craniomaxillofacial trauma. J Oral Maxillofac Surg. 2004; 62:676–684. PMID: 15170277.
Article3. Berne JD, Reuland KR, Villarreal DH, McGovern TM, Rowe SA, Norwood SH. Internal carotid artery stenting for blunt carotid artery injuries with an associated pseudoaneurysm. J Trauma. 2008; 64:398–405. PMID: 18301205.
Article4. Cosan TE, Arslantas A, Guner AI, Vural M, Kaya T, Tel E. Injury caused by deeply penetrating knife blade lodged in infratemporal fossa. Eur J Emerg Med. 2001; 8:51–54. PMID: 11314822.
Article5. Ferguson E, Dennis JW, Vu JH, Frykberg ER. Redefining the role of arterial imaging in the management of penetrating zone 3 neck injuries. Vascular. 2005; 13:158–163. PMID: 15996373.
Article6. Gracias VH, Reilly PM, Philpott J, Klein WP, Lee SY, Singer M, et al. Computed tomography in the evaluation of penetrating neck trauma: a preliminary study. Arch Surg. 2001; 136:1231–1235. PMID: 11695963.7. Herrera DA, Vargas SA, Dublin AB. Endovascular treatment of penetrating traumatic injuries of the extracranial carotid artery. J Vasc Interv Radiol. 2011; 22:28–33. PMID: 21109458.
Article8. Kazim SF, Shamim MS, Tahir MZ, Enam SA, Waheed S. Management of penetrating brain injury. J Emerg Trauma Shock. 2011; 4:395–402. PMID: 21887033.
Article9. Liu WH, Chiang YH, Hsieh CT, Sun JM, Hsia CC. Transorbital penetrating brain injury by branchlet: a rare case. J Emerg Med. 2011; 41:482–485. PMID: 18950975.
Article10. Mahmoodie M, Sanei B, Moazeni-Bistgani M, Namgar M. Penetrating neck trauma: review of 192 cases. Arch Trauma Res. 2012; 1:14–18. PMID: 24719835.
Article11. Meirowsky AM, Caveness WF, Dillon JD, Rish BL, Mohr JP, Kistler JP, et al. Cerebrospinal fluid fistulas complicating missile wounds of the brain. J Neurosurg. 1981; 54:44–48. PMID: 7463119.
Article12. Saito N, Hito R, Burke PA, Sakai O. Imaging of penetrating injuries of the head and neck: current practice at a level I trauma center in the United States. Keio J Med. 2014; 63:23–33. PMID: 24965876.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of the Common Carotid Artery Penetrating Injury by Grass Cutter Fragment
- A Case of the Zone III Neck Injury by Impalement of a Metal Stick
- Posterior Inferior Cerebellar Artery Aneurysm Associated with Posterior Fossa Arteriovenous Malformation: Report of Three Cases: Case Report
- Anesthetic management of penetrating neck injury patient with embedded knife: A case report
- Penetrating injury of face and neck with the vertebral artery injury: a case report
