Ann Rehabil Med.
2016 Aug;40(4):745-750. 10.5535/arm.2016.40.4.745.
A Comprehensive Rehabilitation Approach in a Patient With Serious Neuropsychiatric Systemic Lupus Erythematosus
- Affiliations
-
- 1Department of Physical Medicine and Rehabilitation, Soonchunhyang University Hospital, Seoul, Korea. yoonhee.choi83@gmail.com
- KMID: 2356662
- DOI: http://doi.org/10.5535/arm.2016.40.4.745
Abstract
- Neuropsychiatric systemic lupus erythematosus (NPSLE) involves the central and peripheral nervous system in patients with systemic lupus erythematosus (SLE). It is essential to specify the problems faced by patients with NPSLE because it causes diverse disabilities and impairs quality of life. After performing a comprehensive evaluation, tailored management should be provided for the patient's specific problems. We report here the case of a 30-year-old female with SLE who experienced serious neuropsychiatric symptoms cerebral infarction followed by posterior reversible encephalopathy syndrome and peripheral polyneuropathy. We systemically assessed the patient using the International Classification of Functioning, Disability and Health model as a clinical problem-solving tool and provided comprehensive rehabilitation by focusing on her problems.
Keyword
MeSH Terms
Figure
-
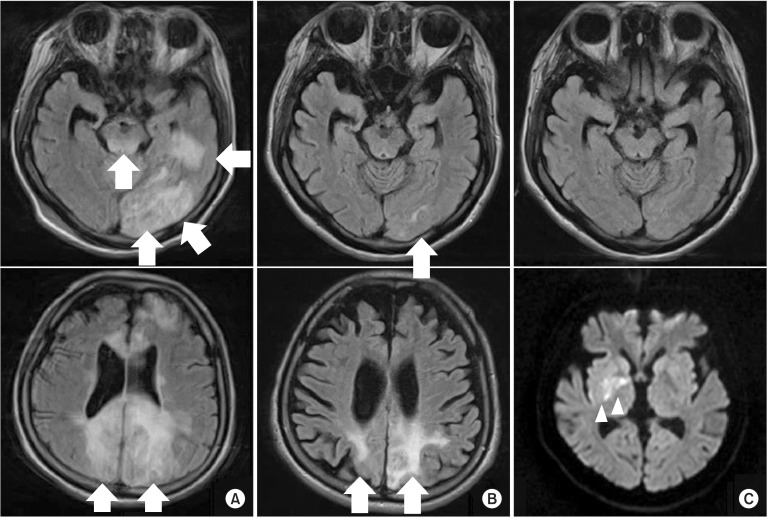
Fig. 1 Sequential brain magnetic resonance images. A T2-fluid attenuation inversion recovery image shows multiple high-signal-intensity lesions in the left temporal and frontal lobes, both occipital lobes, and the midbrain (A). Fifteen days later, the previously noted lesions were markedly resolved (B). Although the previously noted lesions were completely resolved, acute right basal ganglia infarction (arrowheads, C) was seen on brain diffusion magnetic resonance imaging 1 week later.
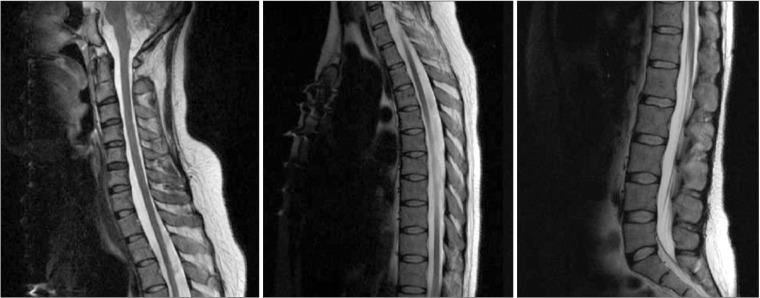
Fig. 2 Whole-spine magnetic resonance image. The cross-sectional area of the whole spinal cord was markedly thin on the sagittal T2-weighted image.
Reference
-
1. Cervera R, Khamashta MA, Font J, Sebastiani GD, Gil A, Lavilla P, et al. Systemic lupus erythematosus: clinical and immunologic patterns of disease expression in a cohort of 1,000 patients. The European Working Party on Systemic Lupus Erythematosus. Medicine (Baltimore). 1993; 72:113–124. PMID: 8479324.2. Hanly JG. Diagnosis and management of neuropsychiatric SLE. Nat Rev Rheumatol. 2014; 10:338–347. PMID: 24514913.
Article3. Lee IH, Ryu YU. Physical therapy combined with corticosteroid intervention for systemic lupus erythematosus with central nervous system involvement: a case report. J Phys Ther Sci. 2014; 26:1839–1841. PMID: 25435712.4. Nencini P, Baruffi MC, Abbate R, Massai G, Amaducci L, Inzitari D. Lupus anticoagulant and anticardiolipin antibodies in young adults with cerebral ischemia. Stroke. 1992; 23:189–193. PMID: 1561646.
Article5. Rauch A, Cieza A, Stucki G. How to apply the International Classification of Functioning, Disability and Health (ICF) for rehabilitation management in clinical practice. Eur J Phys Rehabil Med. 2008; 44:329–342. PMID: 18762742.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Transverse Myelitis as a First Manifestation of Systemic Lupus Erythematosus
- A Ruptured Aneurysm in a Patient with Systemic Lupus Erythematosus: Case Report
- A Case Of Systemic Lupus Erythematosus Associated With Hyperthyroidism And Severe Retinopathy
- Adalimumab-induced Lupus Erythematosus Profundus in a Rheumatoid Arthritis Patient
- A Case of Lupus Enteritis That Developed during the Treatment of Systemic Lupus Erythematosus
