J Korean Assoc Oral Maxillofac Surg.
2016 Oct;42(5):284-287. 10.5125/jkaoms.2016.42.5.284.
Treatment of nevoid basal cell carcinoma syndrome: a case report
- Affiliations
-
- 1Department of Oral and Maxillofacial Surgery, School of Dentistry, Chosun University, Gwangju, Korea. sgckim@chosun.ac.kr
- KMID: 2356255
- DOI: http://doi.org/10.5125/jkaoms.2016.42.5.284
Abstract
- Nevoid basal cell carcinoma syndrome (NBCCS), also known as Gorlin syndrome, is characterized by various embryological deformities and carcinoma formation. It is caused by PTCHI gene mutations and is autosomal dominantly inherited. Some of the main symptoms of NBCCS are multiple basal cell carcinomas, multiple keratocystic odontogenic tumors (KCOTs) of the mandible, hyperkeratosis of the palmar and plantar, skeletal deformity, calcification of the falx cerebri, and facial defomity. Recurrent KCOT is the main symptom of NBCCS and is present in approximately 90% of patients. In NBCCS, KCOTs typically occur in multiples. KCOTs can be detected in patients under the age of 10, and new and recurring cysts develop until approximately the age of 30. The postoperation recurrence rate is approximately 60%. This case report presents a 14-year-old female patient with a chief complaint of a cyst found in the maxilla and mandible. The patient was diagnosed with NBCCS, and following treatment of marsupialization and enucleation, the clinical results were satisfactory.
Keyword
MeSH Terms
Figure
-

Fig. 1 Initial panoramic radiograph of a 14-year-old woman shows a right mandibular cystic lesion and haziness in the left maxillary sinus.
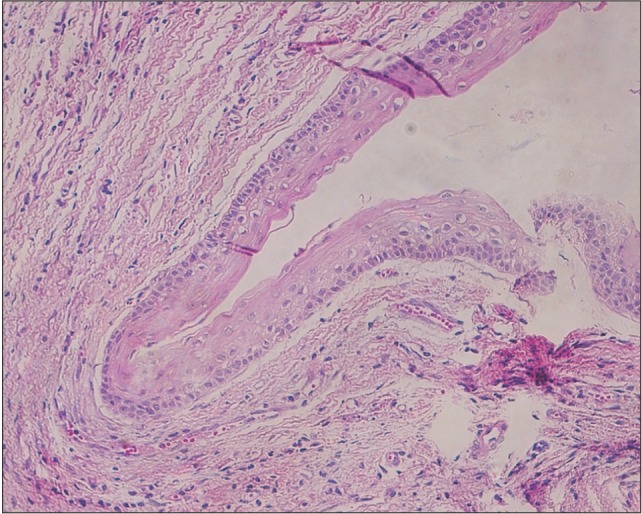
Fig. 2 Micrograph reveals a stratified epithelium lining with the connective tissue stroma of keratocystic odontogenic tumor (H&E staining, ×200).

Fig. 3 Chest PA shows right 4th bifid rib.
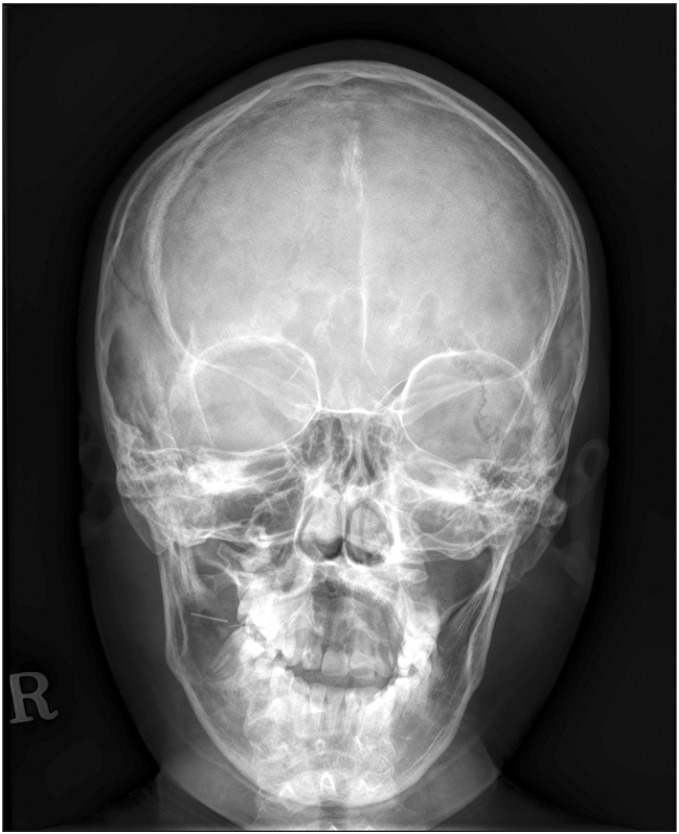
Fig. 4 Skull PA shows calcification of the falx cerebri.

Fig. 5 Water's view radiograph shows calcification of the falx cerebri.

Fig. 6 The panoramic radiographic shows a decrease in the size of the right mandibular cystic lesion after 7 months of decompression.

Fig. 7 The panoramic radiographic shows that the right mandibular lesion has healed well 4.5 years after the first surgery.
Reference
-
1. Gorlin RJ. Nevoid basal cell carcinoma syndrome. Dermatol Clin. 1995; 13:113–125. PMID: 7712637.
Article2. Manfredi M, Vescovi P, Bonanini M, Porter S. Nevoid basal cell carcinoma syndrome: a review of the literature. Int J Oral Maxillofac Surg. 2004; 33:117–124. PMID: 15050066.
Article3. Bakaeen G, Rajab LD, Sawair FA, Hamdan MA, Dallal ND. Nevoid basal cell carcinoma syndrome: a review of the literature and a report of a case. Int J Paediatr Dent. 2004; 14:279–287. PMID: 15242385.
Article4. Evans DG, Ladusans EJ, Rimmer S, Burnell LD, Thakker N, Farndon PA. Complications of the naevoid basal cell carcinoma syndrome: results of a population based study. J Med Genet. 1993; 30:460–464. PMID: 8326488.
Article5. Gorlin RJ, Goltz RW. Multiple nevoid basal-cell epithelioma, jaw cysts and bifid rib. A syndrome. N Engl J Med. 1960; 262:908–912. PMID: 13851319.6. Gorlin RJ. Nevoid basal cell carcinoma (Gorlin) syndrome: unanswered issues. J Lab Clin Med. 1999; 134:551–552. PMID: 10595780.
Article7. Kakarantza-Angelopoulou E, Nicolatou O. Odontogenic keratocysts: clinicopathologic study of 87 cases. J Oral Maxillofac Surg. 1990; 48:593–599. discussion 599-600. PMID: 2187964.8. Kimonis VE, Goldstein AM, Pastakia B, Yang ML, Kase R, DiGiovanna JJ, et al. Clinical manifestations in 105 persons with nevoid basal cell carcinoma syndrome. Am J Med Genet. 1997; 69:299–308. PMID: 9096761.
Article9. Goldstein AM, Pastakia B, DiGiovanna JJ, Poliak S, Santucci S, Kase R, et al. Clinical findings in two African-American families with the nevoid basal cell carcinoma syndrome (NBCC). Am J Med Genet. 1994; 50:272–281. PMID: 8042672.
Article10. Ahn SG, Lim YS, Kim DK, Kim SG, Lee SH, Yoon JH. Nevoid basal cell carcinoma syndrome: a retrospective analysis of 33 affected Korean individuals. Int J Oral Maxillofac Surg. 2004; 33:458–462. PMID: 15183409.
Article11. Gorlin RJ. Nevoid basal-cell carcinoma syndrome. Medicine (Baltimore). 1987; 66:98–113. PMID: 3547011.
Article12. Lo Muzio L. Nevoid basal cell carcinoma syndrome (Gorlin syndrome). Orphanet J Rare Dis. 2008; 3:32. PMID: 19032739.
Article13. Littler BO. Gorlin's syndrome and the heart. Br J Oral Surg. 1979; 17:135–146. PMID: 298837.
Article14. Ozkan L, Aksoy S, Orhan K, Cetiner S, Uyanik LO, Buhara O, et al. Case report: multiple keratocystic odontogenic tumour in a non-syndromal pediatric patient. Eur J Paediatr Dent. 2014; 15(2 Suppl):241–244. PMID: 25101513.15. Vedtofte P, Praetorius F. Recurrence of the odontogenic keratocyst in relation to clinical and histological features. A 20-year follow-up study of 72 patients. Int J Oral Surg. 1979; 8:412–420. PMID: 120338.16. Donatsky O, Hjørting-Hansen E. Recurrence of the odontogenic keratocyst in 13 patients with the nevoid basal cell carcinoma syndrome. A 6-year follow-up. Int J Oral Surg. 1980; 9:173–179. PMID: 6777316.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Two Cases of Nevoid Basal Cell CarcinomaSyndrome in One Family
- Nevoid Basal Cell Carcinoma Syndrome: A Case Report and Literature Review
- A Case of Basal Cell Nevus Syndrome with Odontogenic Keratocyst
- A Case of Multiple Basal Cell Carcinomas in Nevoid Basal Cell Carcinoma Syndrome
- Nevoid Basal Cell Carcinoma Syndrome on Scalp: A Rare Case Report
