Carbohydrate-electrolyte drinks exhibit risks for human enamel surface loss
- Affiliations
-
- 1Operative Dentistry Division, Department of General Dentistry, University of Maryland Dental School, Baltimore, MD, USA. mmelo@umaryland.edu
- 2Division of Operative Dentistry, School of Dentistry, University of Fortaleza, Edson Queiroz Foundation, Fortaleza, CE, Brazil.
- 3School of Dentistry, Centro Universitário Christus - Unichristus, Fortaleza, CE, Brazil.
- 4Postgraduate Program in Dentistry, Faculty of Pharmacy, Dentistry and Nursing, Federal University of Ceará, Fortaleza, CE, Brazil.
- KMID: 2356000
- DOI: http://doi.org/10.5395/rde.2016.41.4.246
Abstract
OBJECTIVES
The aim of this investigation was to give insights into the impact of carbohydrate-electrolyte drinks on the likely capacity of enamel surface dissolution and the influence of human saliva exposure as a biological protective factor.
MATERIALS AND METHODS
The pH, titratable acidity (TA) to pH 7.0, and buffer capacity (β) of common beverages ingested by patients under physical activity were analyzed. Then, we randomly distributed 50 specimens of human enamel into 5 groups. Processed and natural coconut water served as controls for testing three carbohydrate-electrolyte drinks. In all specimens, we measured surface microhardness (Knoop hardness numbers) and enamel loss (profilometry, µm) for baseline and after simulated intake cycling exposure model. We also prepared areas of specimens to be exposed to human saliva overnight prior to the simulated intake cycling exposure. The cycles were performed by alternated immersions in beverages and artificial saliva. ANOVA two-way and Tukey HDS tests were used.
RESULTS
The range of pH, TA, and β were 2.85 - 4.81, 8.33 - 46.66 mM/L and 3.48 - 10.25 mM/L × pH, respectively. The highest capacity of enamel surface dissolution was found for commercially available sports drinks for all variables. Single time human saliva exposure failed to significantly promote protective effect for the acidic attack of beverages.
CONCLUSIONS
In this study, carbohydrate-electrolyte drinks usually consumed during endurance training may have a greater capacity of dissolution of enamel surface depending on their physicochemical proprieties associated with pH and titratable acidity.
Keyword
MeSH Terms
Figure
-
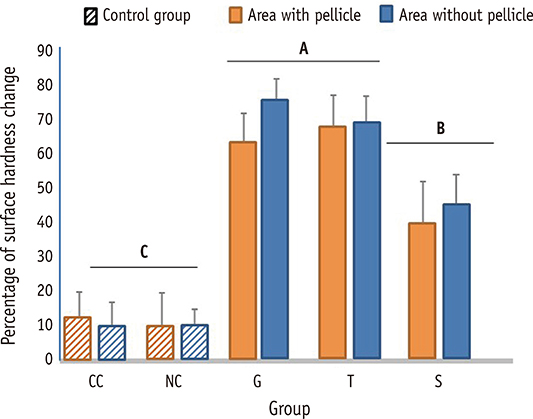
Figure 1 Mean and standard deviation of %SHC considering the presence and absence of acquired pellicle. Different letters correspond to a significant statistic difference among the groups of tested carbohydrate-electrolyte drinks (p < 0.05) and the bars represents that results are statistically similar when the comparison of the area covered with or without in vitro whole-saliva based pellicle. CC, commercial coconut water (control); NC, natural coconut water (control); G, carbohydrate-electrolyte drink (Gatorade); T, carbohydrate-electrolyte drink (Taeq); S, carbohydrate-electrolyte drink (SUUM).
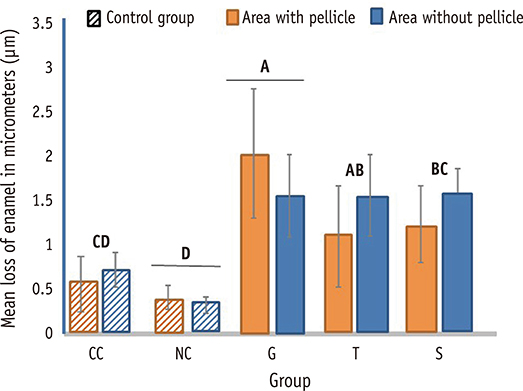
Figure 2 Mean and standard deviation of wear (µm) considering the presence and absence of acquired pellicle. Different letters correspond to a significant statistic difference among the groups of tested carbohydrate-electrolyte drinks (p < 0.05) and the bars represents that results are statistically similar when the comparison of the area covered with or without in vitro whole-saliva based pellicle. CC, commercial coconut water (control); NC, natural coconut water (control); G, carbohydrate-electrolyte drink (Gatorade); T, carbohydrate-electrolyte drink (Taeq); S, carbohydrate-electrolyte drink (SUUM).
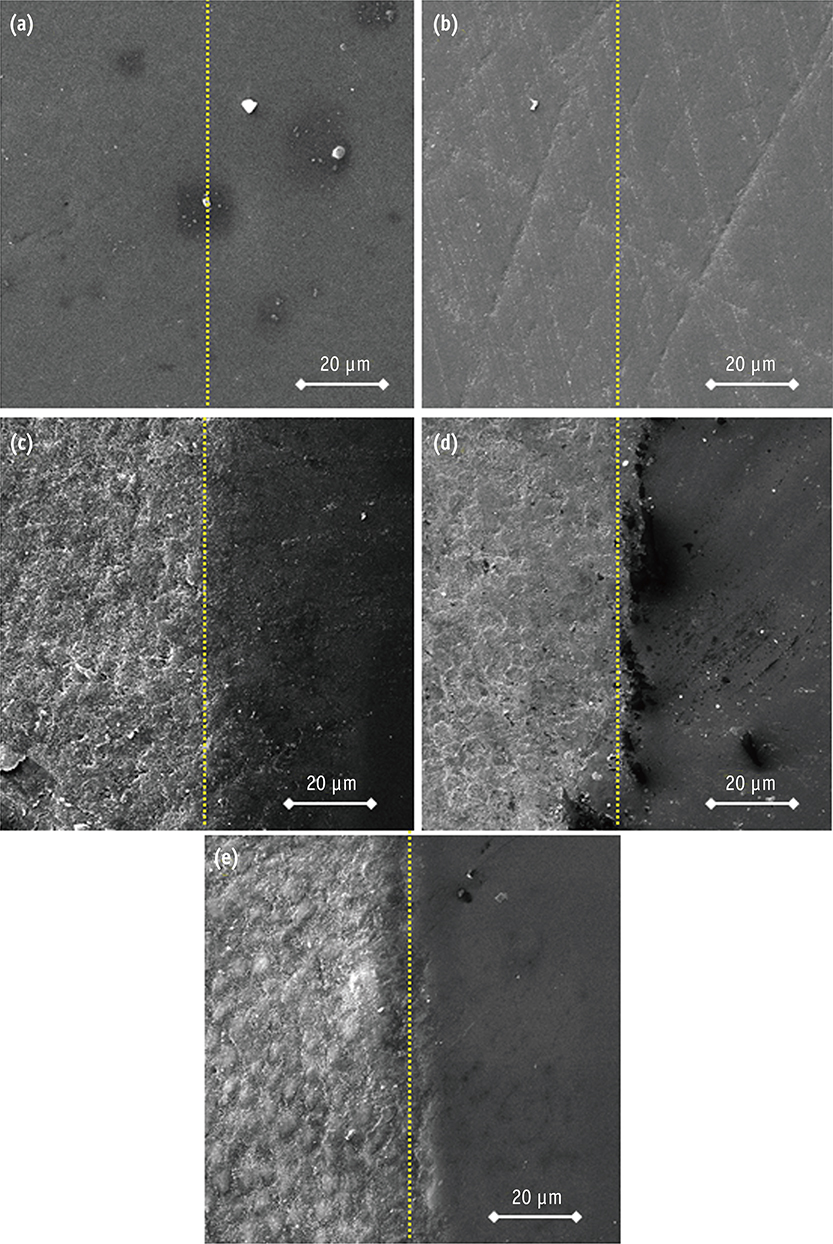
Figure 3 Representative scanning electron micrographs (SEM) of the enamel interface between control (right-hand side) and eroded slab surfaces (left-hand side) with pellicle presence in the each group (×1,500).
Reference
-
1. Ashley P, Di Iorio A, Cole E, Tanday A, Needleman I. Oral health of elite athletes and association with performance: a systematic review. Br J Sports Med. 2015; 49:14–19.
Article2. Ganio MS, Klau JF, Lee EC, Yeargin SW, McDermott BP, Buyckx M, Maresh CM, Armstrong LE. Effect of various carbohydrate-electrolyte fluids on cycling performance and maximal voluntary contraction. Int J Sport Nutr Exerc Metab. 2010; 20:104–114.
Article3. Baker LB, Rollo I, Stein KW, Jeukendrup AE. Acute effects of carbohydrate supplementation on intermittent sports performance. Nutrients. 2015; 7:5733–5763.
Article4. de Sousa MV, Simões HG, Oshiiwa M, Rogero MM, Tirapegui J. Effects of acute carbohydrate supplementation during sessions of high-intensity intermittent exercise. Eur J Appl Physiol. 2007; 99:57–63.
Article5. Nicholas CW, Tsintzas K, Boobis L, Williams C. Carbohydrate-electrolyte ingestion during intermittent high-intensity running. Med Sci Sports Exerc. 1999; 31:1280–1286.
Article6. Lussi A, Jaeggi T, Zero D. The role of diet in the aetiology of dental erosion. Caries Res. 2004; 38:34–44.
Article7. Frese C, Frese F, Kuhlmann S, Saure D, Reljic D, Staehle HJ, Wolff D. Effect of endurance training on dental erosion, caries, and saliva. Scand J Med Sci Sports. 2015; 25:e319–e326.
Article8. Jeukendrup AE. Carbohydrate intake during exercise and performance. Nutrition. 2004; 20:669–677.
Article9. Passos VF, Melo MA, Vasconcellos AA, Rodrigues LK, Santiago SL. Comparison of methods for quantifying dental wear caused by erosion and abrasion. Microsc Res Tech. 2013; 76:178–183.
Article10. Shokouhinejad N, Jafargholizadeh L, Khoshkhounejad M, Nekoofar MH, Raoof M. Surface microhardness of three thicknesses of mineral trioxide aggregate in different setting conditions. Restor Dent Endod. 2014; 39:253–257.
Article11. Park S, Onufrak S, Blanck HM, Sherry B. Characteristics associated with consumption of sports and energy drinks among US adults: National Health Interview Survey, 2010. J Acad Nutr Diet. 2013; 113:112–119.
Article12. Li H, Zou Y, Ding G. Dietary factors associated with dental erosion: a meta-analysis. PLoS One. 2012; 7:e42626.
Article13. Coombes JS. Sports drinks and dental erosion. Am J Dent. 2005; 18:101–104.14. Bartlett D. Etiology and prevention of acid erosion. Compend Contin Educ Dent. 2009; 30:616–620.15. Lussi A, Jaeggi T. Erosion-diagnosis and risk factors. Clin Oral Investig. 2008; 12:Suppl 1. S5–S13.
Article16. Bartlett DW, Fares J, Shirodaria S, Chiu K, Ahmad N, Sherriff M. The association of tooth wear, diet and dietary habits in adults aged 18-30 years old. J Dent. 2011; 39:811–816.
Article17. Richards D. Impact of diet on tooth erosion. Evid Based Dent. 2016; 17:40.
Article18. Salas MM, Nascimento GG, Vargas-Ferreira F, Tarquinio SB, Huysmans MC, Demarco FF. Diet influenced tooth erosion prevalence in children and adolescents: Results of a meta-analysis and meta-regression. J Dent. 2015; 43:865–875.
Article19. Ehlen LA, Marshall TA, Qian F, Wefel JS, Warren JJ. Acidic beverages increase the risk of in vitro tooth erosion. Nutr Res. 2008; 28:299–303.20. Carvalho TS, Baumann T, Lussi A. In vitro salivary pellicles from adults and children have different protective effects against erosion. Clin Oral Investig. 2016; 01. 22. DOI: 10.1007/s00784-015-1703-1. [Epub ahead of print].21. Voronets J, Lussi A. Thickness of softened human enamel removed by toothbrush abrasion: an in vitro study. Clin Oral Investig. 2010; 14:251–256.
Article22. Nekrashevych Y, Stösser L. Protective influence of experimentally formed salivary pellicle on enamel erosion. An in vitro study. Caries Res. 2003; 37:225–231.
Article23. De Melo MA, Passos VF, Lima JP, Parente GC, Rodrigues LK, Santiago SL. Erosive potential of processed and fresh orange juice on human enamel. J Dent Child (chic). 2015; 82:10–15.24. Peacock OJ, Thompson D, Stokes KA. Voluntary drinking behaviour, fluid balance and psychological affect when ingesting water or a carbohydrate-electrolyte solution during exercise. Appetite. 2012; 58:56–63.
Article25. Ismail I, Singh R, Sirisinghe RG. Rehydration with sodium-enriched coconut water after exercise-induced dehydration. Southeast Asian J Trop Med Public Health. 2007; 38:769–785.26. Jensdottir T, Holbrook P, Nauntofle B, Buchwald C, Bardow A. Immediate erosive potential of cola drinks and orange juices. J Dent Res. 2006; 85:226–230.
Article27. de Carvalho Sales-Peres SH, Magalhães AC, de Andrade Moreira Machado MA, Buzalaf MA. Evaluation of the erosive potential of soft drinks. Eur J Dent. 2007; 1:10–13.
Article28. Zheng J, Huang H, Shi MY, Zheng L, Qian LM, Zhou ZR. In vitro study on the wear behaviour of human tooth enamel in citric acid solution. Wear. 2011; 271:2313–2321.
Article29. Hara AT, Zero DT. Analysis of the erosive potential of calcium-containing acidic beverages. Eur J Oral Sci. 2008; 116:60–65.
Article30. Borges AB, Scaramucci T, Lippert F, Zero DT, Hara AT. Erosion protection by calcium lactate/sodium fluoride rinses under different salivary flows in vitro. Caries Res. 2014; 48:193–199.
Article31. Barbour ME, Parker DM, Allen GC, Jandt KD. Enamel dissolution in citric acid as a function of calcium and phosphate concentrations and degree of saturation with respect to hydroxyapatite. Eur J Oral Sci. 2003; 111:428–433.
Article32. Oh S, Perinpanayagam H, Lee Y, Kum JW, Yoo YJ, Lim SM, Chang SW, Shon WJ, Lee W, Baek SH, Kum KY. Effect of acidic solutions on the microhardness of dentin and set Ortho MTA and their cytotoxicity on murine macrophage. Restor Dent Endod. 2016; 41:12–21.
Article33. Yong JW, Ge L, Ng YF, Tan SN. The chemical composition and biological properties of coconut (Cocos nucifera L.) water. Molecules. 2009; 14:5144–5164.
Article34. Hannig M, Hess NJ, Hoth-Hannig W, De Vrese M. Influence of salivary pellicle formation time on enamel demineralization: an in situ pilot study. Clin Oral Investig. 2003; 7:158–161.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Effect of red vinegar drink on the surface of sound enamel
- Effect of commercial alcoholic drinks on sound enamel surface of bovine teeth
- A comparative study of roughness of enamel surface to various interdental enamel stripping methods in vitro
- A study of enamel demineralization related to bonded orthodontic bracket and improved method of enamel demineralization: in vivo study
- Evaluation of the Potential of Commercial Vitamin Drinks to Induce Tooth Erosion
