A Case of a Desmoid Tumor with an Ureterotumoral Fistula Detected on Renal Scintigraphy
- Affiliations
-
- 1Department of Radiology, Soonchunhyang University Cheonan Hospital, Cheonan, Korea.
- 2Department of Internal Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Korea.
- 3Department of Nuclear Medicine, Soonchunhyang University Cheonan Hospital, Cheonan, Korea. c91300@schmc.ac.kr
- KMID: 2355997
- DOI: http://doi.org/10.3348/jksr.2016.75.5.410
Abstract
- Desmoid tumors are rare benign tumors with aggressive fibroblastic proliferation. Although desmoid tumors do not metastasize, they have locally aggressive features and can cause a urinary fistula. Here, we report a case of a 35-year-old woman with Gardner syndrome who was diagnosed with an intra-abdominal desmoid tumor 1 year previously and who presented with a newly developed cystic mass lesion on a computed tomography scan. The cystic mass lesion was clinically diagnosed as an urinoma from the right ureterotumoral fistula; thus, surgical resection of the mass lesion was planned. However, Tc-99m diethylenetriamine pentaacetic acid renal scintigraphy revealed bilateral ureterotumoral fistulas; hence, the treatment plan was changed to conservative management.
MeSH Terms
Figure
-

Fig. 1 A 35-year-old woman with Gardner syndrome. A. Transaxial CT images of the patient. A histologically confirmed desmoid tumor is located in the small bowel mesentery on preoperative abdomen CT (arrow). B. One year later, contrast-enhanced abdominal CT was performed to evaluate the abdominal pain. The already identified desmoid tumor (arrow) is noted in the small bowel mesentery. C. A new poorly-enhanced cystic mass lesion with an air bubble (arrow) is found in the small bowel mesentery. CT = computed tomography
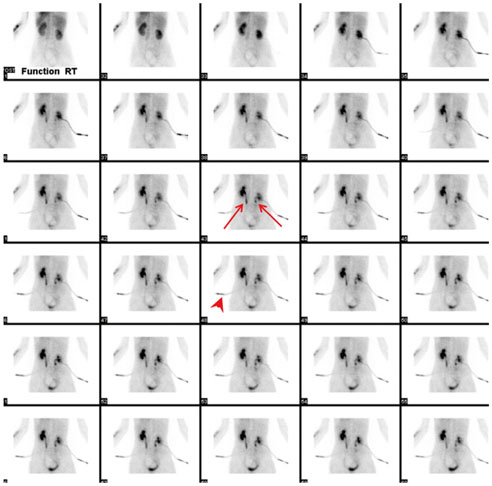
Fig. 2 Excretory phase of Tc-99m DTPA renal scintigraphy. Normal radiotracer uptake into the renal cortex and pelvis is seen with radiotracer uptake in the percutaneous nephrostomy tube in the first row. However, the radiotracer is persistently retained and is detected in bilateral renal pelvis and proximal ureters with a cut-off of radioactivity at bilateral mid-ureters (arrows). Only faint radiotracer activity is seen in bilateral distal ureters and increased radiotracer activity is seen in the percutaneous drainage (PCD) tube (arrowhead). The radiotracer did not accumulate in the cystic mass lesion because of the PCD tube. DTPA = diethylenetriamine pentaacetic acid

Fig. 3 Maximal intensity projection FDG PET/CT scan. PET/CT images were acquired after locking the percutaneous drainage tube. Similar to the renal scintigraphy images, radioactivity is retained in the urine from the renal pelvis to the mid-ureter level in both kidneys. Radioactivity is also detected in the urine in the cystic mass lesion (arrow). The focal FDG activity of the right pubic bone (arrowhead) indicates a traumatic change. CT = computed tomography, FDG = fluorodeoxyglucose, PET = positron emission tomography
Reference
-
1. Escobar C, Munker R, Thomas JO, Li BD, Burton GV. Update on desmoid tumors. Ann Oncol. 2012; 23:562–569.2. Lath C, Khanna PC, Gadewar SB, Agrawal D. Inoperable aggressive mesenteric fibromatosis with ureteric fistula. Case report and literature review. Eur J Radiol. 2006; 59:117–121.3. Kim DU, McQuinn G, Lin E, Lee M. Renographic demonstration of desmoid tumor-ureteral fistula. Clin Nucl Med. 2016; 41:44–45.4. Richard HM 3rd, Thall EH, Mitty H, Gribetz ME, Gelernt I. Desmoid tumor-ureteral fistula in Gardner's syndrome. Urology. 1997; 49:135–138.5. Jung RS, Agarwal K, Sood A, Bhattacharya A, Mittal BR. Hybrid SPECT/CT as a diagnostic modality in suspected urinoma with ambiguous planar Tc99m EC renal scintigraphy. Indian J Nucl Med. 2013; 28:254–255.6. Poyraz NY, Ozdemir E, Keskin M, Türkölmez S. Additional value of SPECT/CT to Tc-99m MAG3 renal scintigraphy in the diagnosis of a patient with ureteroileal fistula. Mol Imaging Radionucl Ther. 2012; 21:84–87.7. Jones IT, Jagelman DG, Fazio VW, Lavery IC, Weakley FL, McGannon E. Desmoid tumors in familial polyposis coli. Ann Surg. 1986; 204:94–97.8. Sportiello DJ, Hoogerland DL. A recurrent pelvic desmoid tumor successfully treated with tamoxifen. Cancer. 1991; 67:1443–1446.9. Kabra V, Chaturvedi P, Pathak KA, deSouza LJ. Mesenteric fibromatosis: a report of three cases and literature review. Indian J Cancer. 2001; 38:133–136.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- A Case of Ileal Mesenteric Desmoid Tumor Resected by Laparoscopic Surgery
- Clinical Experience of Partial Resection of Desmoid Tumor and Perforated Small Bowel for Unresectable Desmoid Tumor with Small Bowel Perforation after IPAA for FAP
- A Case of Nasal Desmoid Tumor
- Desmoid Tumor of the Facet Joint: A Case Report
- A Case of Desmoid Tumor of Rectus Abdominis Muscle Associated with pregnancy
