J Cerebrovasc Endovasc Neurosurg.
2016 Sep;18(3):229-233. 10.7461/jcen.2016.18.3.229.
Results of Endovascular Coil Embolization Treatment for Small (≤ 5 mm) Unruptured Intracranial Aneurysms
- Affiliations
-
- 1Department of Neurosurgery, Presbyterian Medical Center, Jeonju, Korea. lsw1430@gamil.com
- KMID: 2355646
- DOI: http://doi.org/10.7461/jcen.2016.18.3.229
Abstract
OBJECTIVE
Researchers and clinicians have been unable to fully elucidate the natural course of and proper treatment for unruptured intracranial aneurysms (UIAs) smaller than or equal to 5 mm, particularly with regard to whether close observation or surgery is more appropriate. In this retrospective study, we evaluated the safety and efficacy of endovascular coil embolization of small (≤ 5 mm) asymptomatic UIAs by analyzing outcomes and complications associated with the procedure.
MATERIALS AND METHODS
We analyzed data from 150 patients with small asymptomatic UIAs (≤ 5 mm) treated with coil embolization between January 2011 and December 2015. Three-dimensional angiography was used to measure aneurysm size. We evaluated procedure-related morbidity and mortality, immediate post-operative angiographic results, brain computed thomography follow-up results on post-operative day one, and clinical progress.
RESULTS
UIAs occurred primarily in the anterior circulation area (142 cases, 94.67%), though eight patients exhibited UIAs of the posterior circulation. Following coil embolization, aneurysms with complete occlusion were observed in 137 cases (91.3%). Partial occlusion occurred in five cases (3.33%), while the procedure had failed in eight cases (5.33%). Procedure-related morbidity and mortality were five cases (3.33%) and zero cases, respectively.
CONCLUSION
The endovascular treatment of small asymptomatic UIAs is associated with good short-term outcomes without permanent neurologic complications as well as low overall complication and morbidity rates. Thus, the procedure should be considered for patients with smaller asymptomatic UIAs.
MeSH Terms
Figure
-
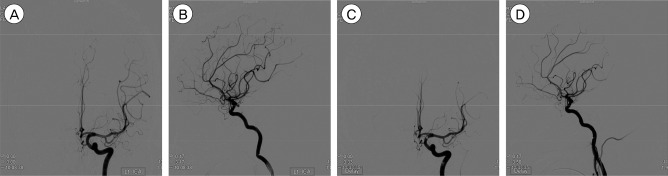
Fig. 1 Transfemoral cerebral angiograms in a 71-year-old male patient. The 3.6 mm × 3.3 mm unruptured intracranial aneurysm (UIA) is visible on the left posterior communicating artery. (A, B) Frontal and lateral views showing pre-embolization UIA. (C, D) Frontal and lateral views showing a totally occluded aneurysmal sac after coil embolization.
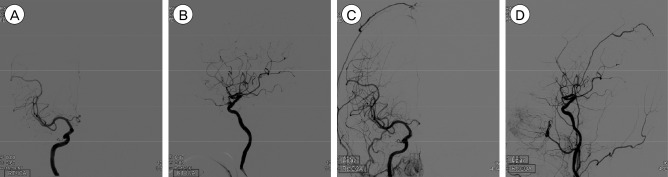
Fig. 2 Transfemoral cerebral angiograms in a 61-year-old female patient. The 4.9 mm × 2.7 mm UIA is visible on the right ophthalmic artery. (A, B) Frontal and lateral views showing pre-embolization UIA. (C, D) Frontal and lateral views showing a partially occluded aneurysmal sac after coil embolization.
Reference
-
1. Byoun HS, Huh W, Oh CW, Bang JS, Hwang G, Kwon OK. Natural history of unruptured intracranial aneurysms: a retrospective single center analysis. J Korean Neurosurg Soc. 2016; 1. 59(1):11–16. PMID: 26885281.2. Im SH, Han MH, Kwon OK, Kwon BJ, Kim SH, Kim JE, et al. Endovascular coil embolization of 435 small asymptomatic unruptured intracranial aneurysms: procedural morbidity and patient outcome. AJNR Am J Neuroradiol. 2009; 1. 30(1):79–84. PMID: 18768715.
Article3. Johnston SC, Wilson CB, Halbach VV, Higashida RT, Dowd CF, McDermott MW, et al. Endovascular and surgical treatment of unruptured cerebral aneurysms: comparison of risks. Ann Neurol. 2000; 7. 48(1):11–19. PMID: 10894211.4. Johnston SC, Zhao S, Dudley RA, Berman MF, Gress DR. Treatment of unruptured cerebral aneurysms in California. Stroke. 2001; 3. 32(3):597–605. PMID: 11239174.
Article5. Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: probability and risk factors for aneurysm rupture. Neurosurg Focus. 2000; 8(5):Preview 1. PMID: 16865812.6. Juvela S, Porras M, Poussa K. Natural history of unruptured intracranial aneurysms: probability of and risk factors for aneurysm rupture. J Neurosurg. 2000; 9. 93(3):379–387. PMID: 10969934.
Article7. Juvela S, Poussa K, Lehto H, Porras M. Natural history of unruptured intracranial aneurysms: a long-term follow-up study. Stroke. 2013; 9. 44(9):2414–2421. PMID: 23868274.
Article8. Lanterna LA, Tredici G, Dimitrov BD, Biroli F. Treatment of unruptured cerebral aneurysms by embolization with guglielmi detachable coils: case-fatality, morbidity, and effectiveness in preventing bleeding--a systematic review of the literature. Neurosurgery. 2004; 10. 55(4):767–775. discussion 775-8. PMID: 15458585.
Article9. Ogilvy CS, Carter BS. Stratification of outcome for surgically treated unruptured intracranial aneurysms. Neurosurgery. 2003; 1. 52(1):82–87. discussion 87-8. PMID: 12493104.
Article10. Sonobe M, Yamazaki T, Yonekura M, Kikuchi H. Small unruptured intracranial aneurysm verification study: SUAVe study, Japan. Stroke. 2010; 9. 41(9):1969–1977. PMID: 20671254.11. Wiebers DO, Whisnant JP, Huston J 3rd, Meissner I, Brown RD Jr, Piepgras DG, et al. Unruptured intracranial aneurysms: natural history, clinical outcome, and risks of surgical and endovascular treatment. Lancet. 2003; 7. 362(9378):103–110. PMID: 12867109.
Article
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unruptured Aneurysms-Endovascular Treatment
- Delayed Complications after Uneventful Coil Embolization of Unruptured Aneurysms : Case Report
- Recent Trends in the Treatment of Cerebral Aneurysms: Comparison between Endovascular Coil Embolization and Surgical Clipping
- Ruptured Very Small Cerebral Aneurysms and the Usefulness of Coil Embolization
- Combined Endovascular and Microsurgical Procedures as Complementary Approaches in the Treatment of a Single Intracranial Aneurysm
