"One-Time" versus Staged Multivessel Intervention in Intermediate to Very High-Risk Patients with Non-ST-Segment Elevation Acute Coronary Syndromes
- Affiliations
-
- 1Department of Cardiology, The Second Hospital of Dalian Medical University, Dalian, Liao Ning, China.
- 2Department of Cardiology, General Hospital of Shenyang Military Region, Shenyang, Liao Ning, China. hanyaling@263.net
- 3Department of Cardiology, Anhui Provincial Hospital, Hefei, Anhui, China.
- KMID: 2355452
- DOI: http://doi.org/10.4070/kcj.2016.46.6.774
Abstract
- BACKGROUND AND OBJECTIVES
To compare clinical outcomes of staged versus "one-time" percutaneous coronary intervention (PCI) in intermediate to very high-risk patients with non-ST-segment elevation acute coronary syndromes (NSTE-ACS) and multivessel coronary disease (MVD).
SUBJECTS AND METHODS
1531 NSTE-ACS patients with multivessel PCI and meeting the criteria of intermediate to very high risk were screened from a prospectively registered database obtained from General Hospital of Shenyang Military Region between 2008 and 2012. They were categorized into "one-time" PCI (n=859) and staged PCI (n=672) according to intervention strategy. The primary outcomes included a 3-year major adverse cardiac event (MACE), a composite of cardiac death, myocardial infarction (MI), and target vessel revascularization.
RESULTS
At 3 years, no significant differences in MACE (20.8% vs. 19.7%, p=0.608) and cardiac death/MI (7.1% vs. 9.1%, p=0.129) were observed between the two groups. After propensity score matching, there was no statistical significance in MACE (18.9% vs. 21.8%, p=0.249); whereas cardiac death/MI was significantly lower in the staged PCI group (7.0% vs.11.1%, p=0.033). Ninety-day landmark analysis showed that the staged PCI group had a lower 90-day incidence of MACE (1.2% vs. 3.3%, p= 0.037) and cardiac death/MI (0.7% vs. 2.6%, p=0.031). For the 90-day to 3-year follow-up period, the incidences of MACE (17.9% vs. 19.1%, p=0.641) and cardiac death/MI (6.3% vs. 8.7%, p=0.191) were similar in both groups.
CONCLUSION
In intermediate- to very high-risk NSTE-ACS patients with MVD, staged PCI is superior to "one-time" PCI in terms of cardiac death/MI.
MeSH Terms
Figure
-
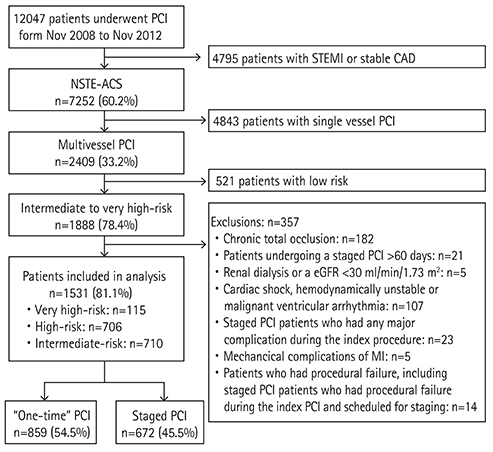
Fig. 1 Patient flow diagram. PCI: percutaneous coronary intervention, STEMI: ST-segment elevation myocardial infarction, CAD: coronary artery disease, NSTE-ACS: non–ST-segment elevation acute coronary syndromes, eGFR: estimated glomerular filtration rate.
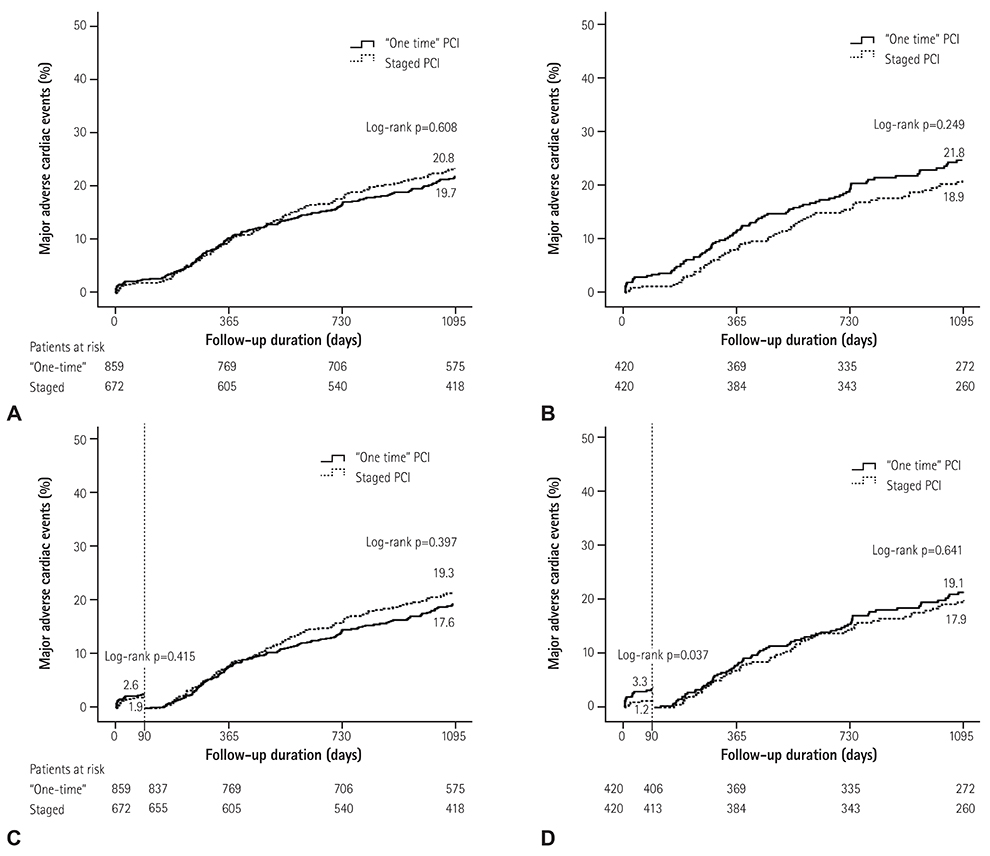
Fig. 2 Kaplan-Meier assessment of MACE for unadjusted (A) and propensity score matched (B) patients; 90-day landmark analysis of MACE for unadjusted (C) and propensity score matched (D) patients. MACE: major adverse cardiac events, PCI: percutaneous coronary intervention.
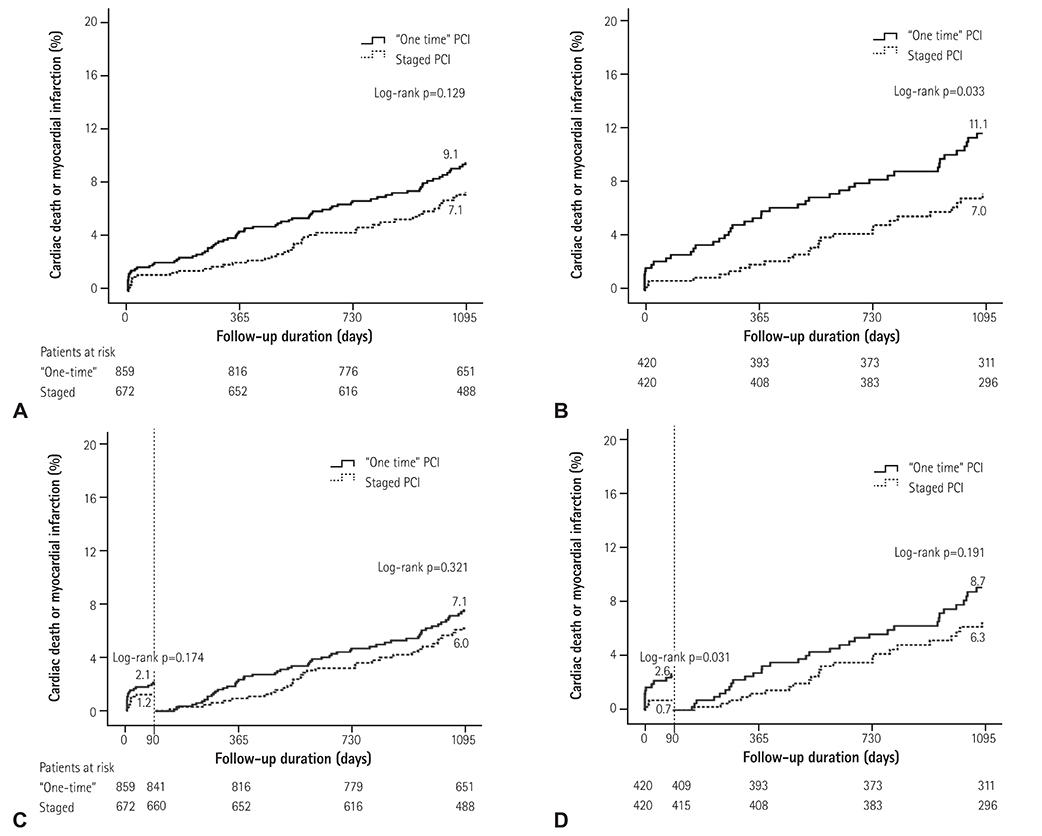
Fig. 3 Kaplan-Meier assessment for the composite of cardiac death or MI for unadjusted (A) and propensity score matched(B) patients; 90-day landmark analysis of the composite of cardiac death or MI for unadjusted (C) and propensity score matched (D) patients. PCI: percutaneous coronary intervention. MI: myocardial infarction.
Cited by 1 articles
-
Complete Versus Culprit-Only Revascularization for ST-Segment Elevation Myocardial Infarction and Multivessel Disease in the 2nd Generation Drug-Eluting Stent Era: Data from the INTERSTELLAR Registry
Sung Woo Kwon, Sang-Don Park, Jeonggeun Moon, Pyung Chun Oh, Ho-Jun Jang, Hyun Woo Park, Tae-Hoon Kim, Kyounghoon Lee, Jon Suh, WoongChol Kang
Korean Circ J. 2018;48(11):989-999. doi: 10.4070/kcj.2017.0387.
Reference
-
1. Authors/Task Force members. Windecker S, Kolh P, et al. 2014 ESC/EACTS Guidelines on myocardial revascularization: The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS) Developed with the special contribution of the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2014; 35:2541–2619.2. Roffi M, Patrono C, Collet JP, et al. 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Eur Heart J. 2016; 37:267–315.3. Amsterdam EA, Wenger NK, Brindis RG, et al. 2014 AHA/ACC Guideline for the Management of Patients with Non-ST-Elevation Acute Coronary Syndromes: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014; 64:e139–e228.4. Loscalzo J, Longo DL, Fauci AS, et al. Unstable angina and non-STelevation myocardial infarction. In : Cannon CP, editor. Harrison Cardiovascular Medicine. New York: McGraw-Hill Education;2013. p. 407–414.5. Shishehbor MH, Lauer MS, Singh IM, et al. In unstable angina or non-ST-segment acute coronary syndrome, should patients with multivessel coronary artery disease undergo multivessel or culprit-only stenting? J Am Coll Cardiol. 2007; 49:849–854.6. Kim MC, Jeong MH, Ahn Y, et al. What is optimal revascularization strategy in patients with multivessel coronary artery disease in non-ST-elevation myocardial infarction? Multivessel or culprit-only revascularization. Int J Cardiol. 2011; 153:148–153.7. Brener SJ, Milford-Beland S, Roe MT, et al. Culprit-only or multivessel revascularization in patients with acute coronary syndromes: an American College of Cardiology National Cardiovascular Database Registry report. Am Heart J. 2008; 155:140–146.8. Zapata GO, Lasave LI, Kozak F, et al. Culprit-only or multivessel percutaneous coronary stenting in patients with non-ST-segment elevation acute coronary syndromes: one-year follow-up. J Interv Cardiol. 2009; 22:329–335.9. Ambrose JA, Winters SL, Stern A, et al. Angiographic morphology and the pathogenesis of unstable angina pectoris. J Am Coll Cardiol. 1985; 5:609–616.10. Kerensky RA, Wade M, Deedwania P, Boden WE, Pepine CJ. Revisiting the culprit lesion in non-Q-wave myocardial infarction. Results from the VANQWISH trial angiographic core laboratory. J Am Coll Cardiol. 2002; 39:1456–1463.11. Goldstein JA, Demetriou D, Grines CL, Pica M, Shoukfeh M, O'Neill WW. Multiple complex coronary plaques in patients with acute myocardial infarction. N Engl J Med. 2000; 343:915–922.12. Luczak D, Majda W, Dabrowski R, et al. Prognostic importance of the extent of coronary revascularisation in patients with acute coronary syndromes and multivessel disease: one-year prospective follow-up. Kardiol Pol. 2015; 73:159–166.13. Ma YC, Zuo L, Chen JH, et al. Modified glomerular filtration rate estimating equation for Chinese patients with chronic kidney disease. J Am Soc Nephrol. 2006; 17:2937–2944.14. XH W, XF L. Diagnostics. 8th ed. Beijing: People's Medical Publishing House;2013.15. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012; 60:1581–1598.16. Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007; 115:2344–2351.17. Dangas GD, George JC, Weintraub W, Popma JJ. Timing of staged percutaneous coronary intervention in multivessel coronary artery disease. JACC Cardiovasc Interv. 2010; 3:1096–1099.18. Hannan EL, Samadashvili Z, Walford G, et al. Staged versus one-time complete revascularization with percutaneous coronary intervention for multivessel coronary artery disease patients without ST-elevation myocardial infarction. Circ Cardiovasc Interv. 2013; 6:12–20.19. Ohashi Y, Kawashima S, Mori T, et al. Soluble CD40 ligand and interleukin-6 in the coronary circulation after acute myocardial infarction. Int J Cardiol. 2006; 112:52–58.20. Kereiakes DJ, Gurbel PA. Peri-procedural platelet function and platelet inhibition in percutaneous coronary intervention. JACC Cardiovasc Interv. 2008; 1:111–121.21. Chan MY, Andreotti F, Becker RC. Hypercoagulable states in cardiovascular disease. Circulation. 2008; 118:2286–2297.22. Brummel-Ziedins K, Undas A, Orfeo T, et al. Thrombin generation in acute coronary syndrome and stable coronary artery disease: dependence on plasma factor composition. J Thromb Haemost. 2008; 6:104–110.23. Di Mario C, Mara S, Flavio A, et al. Single vs multivessel treatment during primary angioplasty: results of the multicentre randomised HEpacoat for cuLPrit or multivessel stenting for Acute Myocardial Infarction (HELP AMI) Study. Int J Cardiovasc Intervent. 2004; 6:128–133.24. Gasior P, Desperak P, Gierlaszynska K, et al. Percutaneous coronary intervention in treatment of multivessel coronary artery disease in patients with non-ST-segment elevation acute coronary syndrome. Postepy Kardiol Interwencyjnej. 2013; 9:136–145.25. Zimarino M, Curzen N, Cicchitti V, De Caterina R. The adequacy of myocardial revascularization in patients with multivessel coronary artery disease. Int J Cardiol. 2013; 168:1748–1757.26. Jernberg T, Hasvold P, Henriksson M, Hjelm H, Thuresson M, Janzon M. Cardiovascular risk in post-myocardial infarction patients: nationwide real world data demonstrate the importance of a long-term perspective. Eur Heart J. 2015; 36:1163–1170.27. Marso SP, McGuire DK. Coronary revascularization strategies in patients with diabetes and multivessel coronary artery disease: has the final chapter been written? J Am Coll Cardiol. 2014; 64:1198–1201.28. Elbarouni B, Ismaeil N, Yan RT, et al. Temporal changes in the management and outcome of Canadian diabetic patients hospitalized for non-ST-elevation acute coronary syndromes. Am Heart J. 2011; 162:347–355.e1.29. Abu-Assi E, Ferreira-Gonzalez I, Ribera A, et al. "Do GRACE (Global Registry of Acute Coronary events) risk scores still maintain their performance for predicting mortality in the era of contemporary management of acute coronary syndromes?". Am Heart J. 2010; 160:826–834.e1-3.30. Reuter PG, Rouchy C, Cattan S, et al. Early invasive strategy in high-risk acute coronary syndrome without ST-segment elevation. The Sisca randomized trial. Int J Cardiol. 2015; 182:414–418.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Staged versus One-Time Percutaneous Coronary Intervention Strategy for Multivessel Non-ST Segment Elevation Acute Coronary Syndrome
- Current Status of Coronary Intervention in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Coronary Artery Disease
- Optimal Timing of Percutaneous Coronary Intervention for Nonculprit Vessel in Patients with ST-Segment Elevation Myocardial Infarction and Multivessel Disease
- Clinical Significance of Predischarge Treadmill Exercise Test in Patients with Acute Myocardial Infarction
- ST segment
