Narrow-band imaging with magnifying endoscopy for Peyer's patches is useful in predicting the recurrence of remissive patients with ulcerative colitis
- Affiliations
-
- 1Department of Gastroenterology and Hepatology, Osaka University Graduate School of Medicine, Osaka, Japan. hiijima@gh.med.osaka-u.ac.jp
- 2Department of Therapeutics for Inflammatory Bowel Diseases, Osaka University Graduate School of Medicine, Osaka, Japan.
- 3Department of Gastroenterology, Sumitomo Hospital, Osaka, Japan.
- 4Department of Gastroenterological Surgery, Osaka University Graduate School of Medicine, Osaka, Japan.
- 5Department of Gastroenterology, Osaka Rosai Hospital, Osaka, Japan.
- KMID: 2354949
- DOI: http://doi.org/10.5217/ir.2016.14.4.314
Abstract
- BACKGROUND/AIMS
Peyer's patches (PPs) are aggregates of lymphoid follicles that are mainly located in the distal ileum; they play a major role in mucosal immunity. We recently reported that patients with ulcerative colitis (UC) have alterations in PPs that can be detected using narrow-band imaging with magnifying endoscopy (NBI-ME). However, the usefulness of NBI-ME in UC treatment as a whole is still unknown.
METHODS
We collected NBI-ME images of PPs from 67 UC patients who had undergone ileocolonoscopy. We evaluated changes in the villi using the "villi index," which is based on three categories: irregular formation, hyperemia, and altered vascular network pattern. The patients were divided into two groups on the basis of villi index: low (L)- and high (H)-types. We then determined the correlation between morphological alteration of the PPs and various clinical characteristics. In 52 patients who were in clinical remission, we also analyzed the correlation between NBI-ME findings of PPs and clinical recurrence.
RESULTS
The time to clinical recurrence was significantly shorter in remissive UC patients with H-type PPs than in those with L-type PPs (P<0.01). Moreover, PP alterations were not correlated with age, sex, disease duration, clinical activity, endoscopic score, or extent of disease involvement. Multivariate analysis revealed that the existence of H-type PPs was an independent risk factor for clinical recurrence (hazard ratio, 3.3; P<0.01).
CONCLUSIONS
UC patients with morphological alterations in PPs were at high risk of clinical relapse. Therefore, to predict the clinical course of UC, it may be useful to evaluate NBI-ME images of PPs.
MeSH Terms
Figure
-
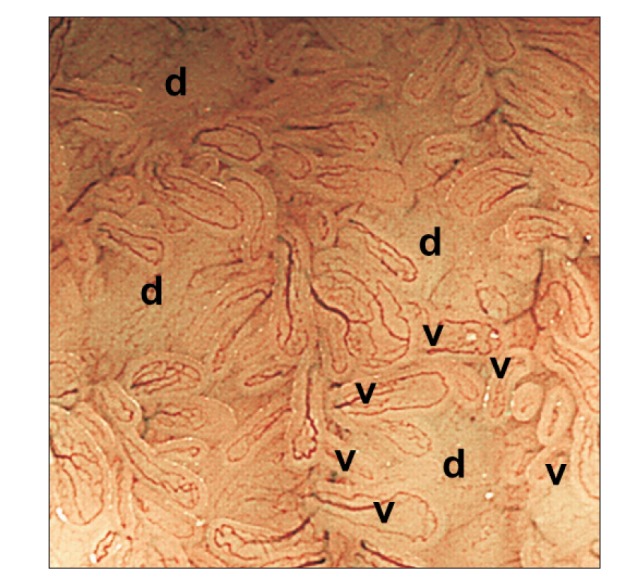
Fig. 1 Narrow-band imaging with magnifying endoscopy allowed us to clearly observe Peyer's patches: aggregates of multiple domes (d) surrounded by villi (v) with semi-circular vessels.
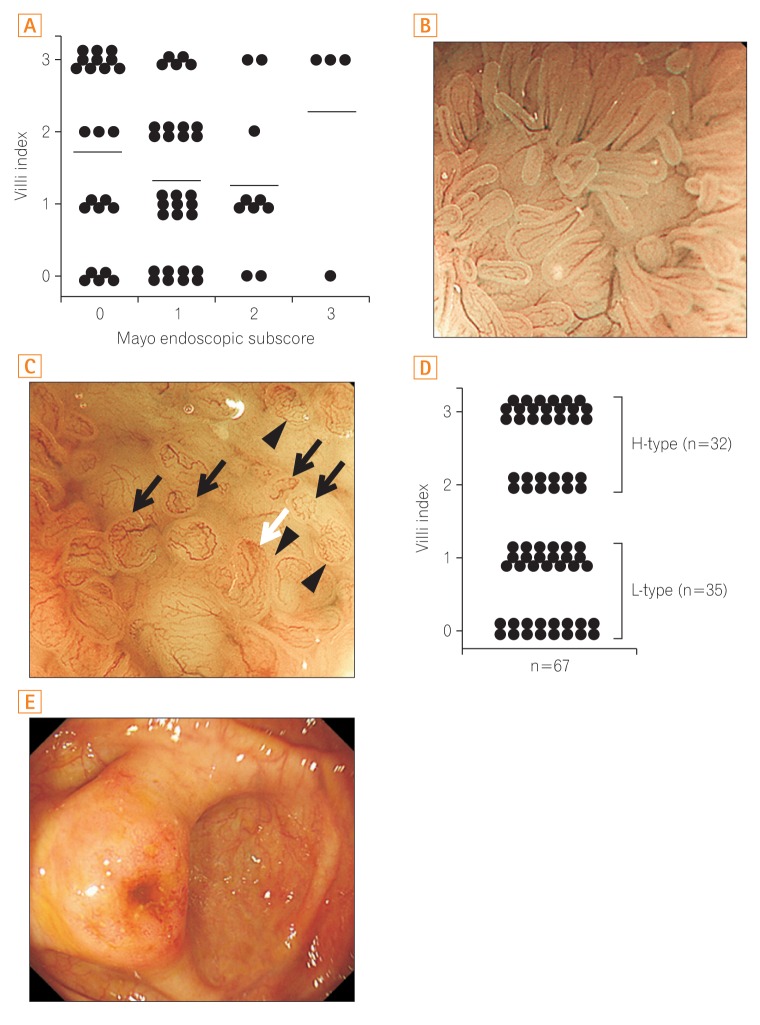
Fig. 2 (A) Scatterplot of the villi index against Mayo endoscopic subscore at the colonoscopy. No correlation was seen between the villi index and the Mayo endoscopic subscore. Bars represent the mean. Representative images of L-type (B) and H-type (C) Peyer's patches (PPs) (black arrows, irregular formation; white arrow, hyperemia; arrowheads, altered vascular network pattern). (D) Evaluation of PPs by narrow-band imaging with magnifying endoscopy in UC patients using the "villi index." Thirty-five patients showed L-type PPs (villi index, 0 or 1), while 32 showed H-type PPs (villi index, 2 or 3). (E) A representative image of the reddish peri-appendiceal mucosa in patients with UC. H-type, high-type; L-type, low-type.
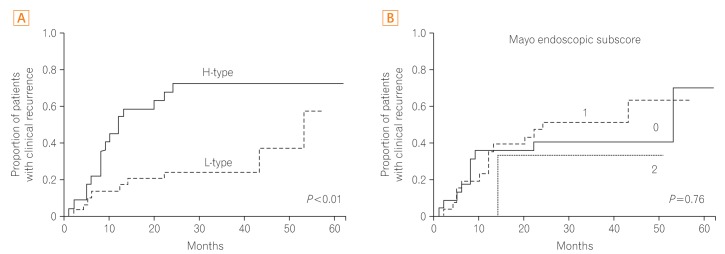
Fig. 3 Results of the Kaplan-Meier survival analysis showing the cumulative proportion of patients who experienced clinical recurrence based on Peyer's patch imaging using narrow-band imaging with magnifying endoscopy (A) and Mayo endoscopic subscore (B). H-type, high-type; L-type, low-type.
Cited by 1 articles
-
Can narrow-band imaging of Peyer's patches predict the recurrence of ulcerative colitis?
Yoon Jae Kim
Intest Res. 2016;14(4):295-296. doi: 10.5217/ir.2016.14.4.295.
Reference
-
1. Iijima H, Takahashi I, Kiyono H. Mucosal immune network in the gut for the control of infectious diseases. Rev Med Virol. 2001; 11:117–133. PMID: 11262530.
Article2. Van Kruiningen HJ, West AB, Freda BJ, Holmes KA. Distribution of Peyer's patches in the distal ileum. Inflamm Bowel Dis. 2002; 8:180–185. PMID: 11979138.
Article3. Leone V, Chang EB, Devkota S. Diet, microbes, and host genetics: the perfect storm in inflammatory bowel diseases. J Gastroenterol. 2013; 48:315–321. PMID: 23475322.
Article4. MacDonald TT, Spencer J, Viney JL, Williams CB, Walker-Smith JA. Selective biopsy of human Peyer's patches during ileal endoscopy. Gastroenterology. 1987; 93:1356–1362. PMID: 3500086.
Article5. Annese V, Daperno M, Rutter MD, et al. European evidence basedconsensus for endoscopy in inflammatory bowel disease. J Crohns Colitis. 2013; 7:982–1018. PMID: 24184171.
Article6. Hiyama S, Iijima H, Shinzaki S, et al. Narrow band imaging with magnifying endoscopy for Peyer's patches in patients with inflammatory bowel disease. Digestion. 2013; 87:269–280. PMID: 23774764.
Article7. Podolsky DK. Inflammatory bowel disease (1). N Engl J Med. 1991; 325:928–937. PMID: 1881418.8. Podolsky DK. Inflammatory bowel disease (2). N Engl J Med. 1991; 325:1008–1016. PMID: 1886623.9. Schroeder KW, Tremaine WJ, Ilstrup DM. Coated oral 5-aminosalicylic acid therapy for mildly to moderately active ulcerative colitis: a randomized study. N Engl J Med. 1987; 317:1625–1629. PMID: 3317057.
Article10. Cornes JS. Number, size, and distribution of Peyer's patches in the human small intestine. Part I: the development of Peyer's patches. Gut. 1965; 6:225–229. PMID: 18668776.
Article11. Nishio Y, Ando T, Maeda O, et al. Pit patterns in rectal mucosa assessed by magnifying colonoscope are predictive of relapse in patients with quiescent ulcerative colitis. Gut. 2006; 55:1768–1773. PMID: 16682428.
Article12. Jauregui-Amezaga A, López-Cerón M, Aceituno M, et al. Accuracy of advanced endoscopy and fecal calprotectin for prediction of relapse in ulcerative colitis: a prospective study. Inflamm Bowel Dis. 2014; 20:1187–1193. PMID: 24874457.
Article13. Ishii H, Isomoto H, Shikuwa S, et al. Peyer's patches in the terminal ileum in ulcerative colitis: magnifying endoscopic findings. J Clin Biochem Nutr. 2010; 46:111–118. PMID: 20216943.
Article14. Gono K, Obi T, Yamaguchi M, et al. Appearance of enhanced tissue features in narrow-band endoscopic imaging. J Biomed Opt. 2004; 9:568–577. PMID: 15189095.
Article15. Kashida H. Usage of narrow band imaging system in the colorectum. Intest Res. 2009; 7:1–7.16. Sands BE. Biomarkers of inflammation in inflammatory bowel disease. Gastroenterology. 2015; 149:1275–1285.e2. PMID: 26166315.17. Liverani E, Scaioli E, Digby RJ, Bellanova M, Belluzzi A. How to predict clinical relapse in inflammatory bowel disease patients. World J Gastroenterol. 2016; 22:1017–1033. PMID: 26811644.18. Henriksen M, Jahnsen J, Lygren I, et al. C-reactive protein: a predictive factor and marker of inflammation in inflammatory bowel disease. Results from a prospective population-based study. Gut. 2008; 57:1518–1523. PMID: 18566104.19. Ardizzone S, Maconi G, Russo A, Imbesi V, Colombo E, Bianchi Porro G. Randomised controlled trial of azathioprine and 5-aminosalicylic acid for treatment of steroid dependent ulcerative colitis. Gut. 2006; 55:47–53. PMID: 15972298.
Article20. Colombel JF, Rutgeerts P, Reinisch W, et al. Early mucosal healing with infliximab is associated with improved long-term clinical outcomes in ulcerative colitis. Gastroenterology. 2011; 141:1194–1201. PMID: 21723220.
Article21. Boal Carvalho P, Dias de Castro F, Rosa B, Moreira MJ, Cotter J. Mucosal healing in ulcerative colitis: when zero is better. J Crohns Colitis. 2016; 10:20–25. PMID: 26438714.22. Haskell H, Andrews CW Jr, Reddy SI, et al. Pathologic features and clinical significance of "backwash" ileitis in ulcerative colitis. Am J Surg Pathol. 2005; 29:1472–1481. PMID: 16224214.
Article23. Park SH, Loftus EV Jr, Yang SK. Appendiceal skip inflammation and ulcerative colitis. Dig Dis Sci. 2014; 59:2050–2057. PMID: 24705639.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Can narrow-band imaging of Peyer's patches predict the recurrence of ulcerative colitis?
- Clinical Usefulness of Magnifying Chromoendoscopy and Magnifying Narrow Band Imaging Endoscopy for Predicting the Submucosal Invasion of Early Colorectal Cancers
- Usefulness of Narrow-Band Imaging in Endoscopic Submucosal Dissection of the Stomach
- Interobserver Agreement in Using Magnifying Narrow Band Imaging System
- Application of artificial intelligence for diagnosis of early gastric cancer based on magnifying endoscopy with narrow-band imaging
