Neurological Deterioration after Decompressive Suboccipital Craniectomy in a Patient with a Brainstem-compressing Thrombosed Giant Aneurysm of the Vertebral Artery
- Affiliations
-
- 1Department of Neurosurgery, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Korea. ns.joonho.chung@gmail.com
- 2Department of Neurosurgery, Dongsan Medical Center, College of Medicine, Keimyung University, Daegu, Korea.
- 3Severance Institute for Vascular and Metabolic Research, Yonsei University College of Medicine, Seoul, Korea.
- KMID: 2354886
- DOI: http://doi.org/10.7461/jcen.2016.18.2.115
Abstract
- We experienced a case of neurological deterioration after decompressive suboccipital craniectomy (DSC) in a patient with a brainstem-compressing thrombosed giant aneurysm of the vertebral artery (VA). A 60-year-old male harboring a thrombosed giant aneurysm (about 4 cm) of the right vertebral artery presented with quadriparesis. We treated the aneurysm by endovascular coil trapping of the right VA and expected the aneurysm to shrink slowly. After 7 days, however, he suffered aggravated symptoms as his aneurysm increased in size due to internal thrombosis. The medulla compression was aggravated, and so we performed DSC with C1 laminectomy. After the third post-operative day, unfortunately, his neurologic symptoms were more aggravated than in the pre-DSC state. Despite of conservative treatment, neurological symptoms did not improve, and microsurgical aneurysmectomy was performed for the medulla decompression. Unfortunately, the post-operative recovery was not as good as anticipated. DSC should not be used to release the brainstem when treating a brainstem-compressing thrombosed giant aneurysm of the VA.
MeSH Terms
Figure
-

Fig. 1 Initial radiographic findings. (A) Computed tomography showed surrounding calcification of the aneurysm wall and (B) magnetic resonance image revealed that the medulla oblongata was squeezed between the aneurysm and occipito-cervical junction.
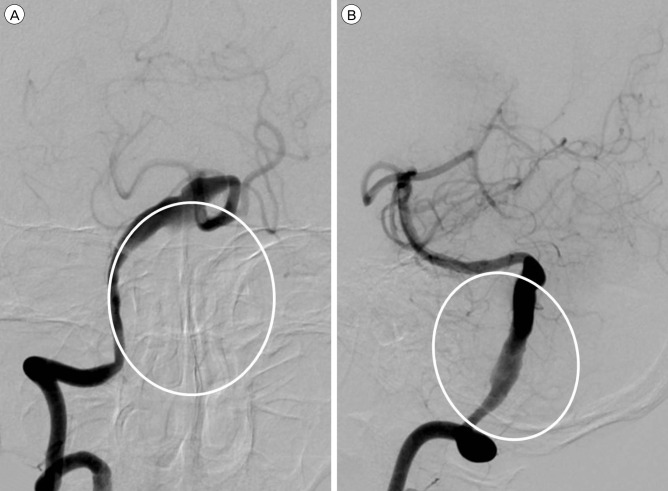
Fig. 2 Cerebral angiography showed fusiform-like dilatation of the right vertebral artery due to the thrombosed sac. The real contour of the aneurysm is indicated by a white circle. (A) Antero-posterior view. (B) Lateral view.

Fig. 3 Follow-up radiographic findings. (A) and (B) The aneurysm size was increased due to internal thrombosis after endovascular trapping of the right vertebral artery, medulla oblongata compression of the aneurysm was aggravated. (C) Decompressive suboccipital craniectomy (DSC) with C1 laminectomy was performed. (D) Magnetic resonance image (MRI) showed more angulation of the medulla oblongata posteriorly with dense high signal changes from the medulla to the upper spinal cord compared to pre-DSC MRI. (E) Microsurgical aneurysmectomy was performed for medulla decompression.
Reference
-
1. Chotai S, Kshettry VR, Lamki T, Ammirati M. Surgical outcomes using wide suboccipital decompression for adult Chiari I malformation with and without syringomyelia. Clin Neurol Neurosurg. 2014; 5. 120:129–135. PMID: 24656777.
Article2. Drake CG. Giant intracranial aneurysms: experience with surgical treatment in 174 patients. Clin Neurosurg. 1979; 26:12–95. PMID: 544122.
Article3. Ganti SR, Steinberger A, McMurtry JG 3rd, Hilal SK. Computed tomographic demonstration of giant aneurysms of the vertebrobasilar system: report of eight cases. Neurosurgery. 1981; 9. 9(3):261–267. PMID: 7301068.4. Hecht ST, Horton JA, Yonas H. Growth of a thrombosed giant vertebral artery aneurysm after parent artery occlusion. AJNR Am J Neuroradiol. 1991; May-Jun. 12(3):449–451. PMID: 2058491.5. Iihara K1, Murao K, Sakai N, Soeda A, Ishibashi-Ueda H, Yutani C, et al. Continued growth of and increased symptoms from a thrombosed giant aneurysm of the vertebral artery after complete endovascular occlusion and trapping: the role of vasa vasorum. Case report. J Neurosurg. 2003; 2. 98(2):407–413. PMID: 12593631.6. Nagahiro S, Takada A, Goto S, Kai Y, Ushio Y. Thrombosed growing giant aneurysms of the vertebral artery: growth mechanism and management. J Neurosurg. 1995; 5. 82(5):796–801. PMID: 7714605.
Article7. Pfefferkorn T, Eppinger U, Linn J, Birnbaum T, Herzog J, Straube A, et al. Long-term outcome after suboccipital decompressive craniectomy for malignant cerebellar infarction. Stroke. 2009; 7. 40(9):3045–3050. PMID: 19574555.
Article8. Ragel BT, Klimo P Jr, Martin JE, Teff RJ, Bakken HE, Armonda RA. Wartime decompressive craniectomy: technique and lessons learned. Neurogurg Focus. 2010; 5. 28(5):E2.
Article9. Ratliff JK, Cooper PR. Cervical laminoplasty: a critical review. J Neurosurg. 2003; 4. 98(3 Suppl):230–238. PMID: 12691377.
Article10. Suda K, Abumi K, Ito M, Shono Y, Kaneda K, Fujiya M. Local kyphosis reduces surgical outcomes of expansive open-door laminoplasty for cervical spondylotic myelophathy. Spine (Phila Pa 1976). 2003; 6. 28(12):1258–1262. PMID: 12811268.11. Sugita K, Kobayashi S, Takemae T, Tanaka Y, Okudera H, Ohsawa M. Giant aneurysms of the vertebral artery. Report of five cases. J Neurosurg. 1988; 6. 68(6):960–966. PMID: 3373290.
- Full Text Links
-
- Actions
-
Cited
- CITED
-
- Close
- Share
-
- Similar articles
-
- Unusual Clinical Course of Giant Vertebral Artery Aneurysm after Proximal Artery Embolization: Case Report
- Surgical Management of Acute Infarction
- Surgical Treatment by the Far Lateral Inferial Suboccipital Approach for the Distal Vertebral Artery Aneurysm
- Strategic Dual Approach for the Management of a Symptomatic Giant Partially Thrombosed Aneurysm at the Basilar Tip - Integrating Intrasaccular Flow Diversion and Endovascular Flow Reversal
- A Case Report of Giant Posterior Inferior Cerebellar Artery Aneurysm Simulating a Posterior Fossa Tumor
